Working with the Institute of Excellence, Pharma’s Q&A issue presents some of the most frequently-asked and relevant questions submitted by members on the ‘AMD webcast,’ answered here by Matt Trinh and Dr Angelica Ly.
Matt Trinh PhD candidate MOptom BOptom (Hons) BSci
Angelica Ly
PhD GradCertOcTher BOptom (Hons) FAAO
Centre for Eye Health and the School of Optometry and Vision Science UNSW
The topic of reticular pseudodrusen (RPD) has seen a surge in research and clinical relevance since its first descriptions in the 1990s.1 We now understand that RPD confer a much higher risk of progression to late age-related macular degeneration (AMD) compared to conventional drusen.2
With the widespread dissemination of multimodal imaging, our definitions of RPD have evolved to incorporate its combined appearance via optical coherence tomography (OCT), near-infrared (NIR), and fundus autofluorescence (FAF). Nevertheless, a universal definition and comprehensive management protocol still evade us. In this Q&A session, we will answer some of the most pertinent questions relating to the diagnosis and management of RPD (with a focus on the application of the Age-Related Eye Disease Study [AREDS] type supplementation).
Q: Can you tell the difference between RPD and conventional drusen by looking at the fundus photo alone?
A: Yes, but don’t do it – you will miss a lot of RPD!
Using coloured fundus photography (CFP) to look for RPD, we’d look for lesions that are typically: 150-250 µm in size; ‘yellowish’ but whiter than conventional soft drusen; flatter and more regular than conventional soft drusen; more visible using the blue-channel; in an interlacing network (although they can occur in isolation).3 However, how many of the above criteria exactly match the appearance of RPD seen in Figure 1?
To accurately diagnose RPD, studies recommend using two or more imaging modalities.
OCT and NIR consistently show the greatest overall sensitivity and specificity for diagnosing RPD (> 90 per cent), followed by fundus autofluorescence (70-90 per cent sensitivity, > 90 per cent specificity).4–7
Overall, OCT and/or NIR should thus be used as the primary modalities to detect RPD. FAF and/or CFP may then be used as supplementary tools to confirm diagnosis.4–8
With further multi-modal imaging, our criteria for defining RPD has evolved significantly beyond what was originally established using CFP:
Using OCT and confirmed through histological studies, RPD are hyperreflective lesions, existing above the RPE, directly beneath the photoreceptors;9–11
Using NIR, RPD are hyporeflective with a mild hyperreflective background, and can be 50-400 µm in size as opposed to earlier descriptions of 125-250 µm;8
Using FAF, RPD typically have a hypo- or iso-fluorescent centre with mild hyperfluorescent borders amongst a reticular, interlacing network.3,12,13
Overall, using a relatively broader scanning area, for example 30 degrees × 25 degrees, will help maximise detection as RPD typically present at the vascular arcades.5
Q: Are RPD exclusive to AMD?
A: Definitely not; up to 35 per cent of RPD occur in aged eyes with no AMD.1,5,14
RPD has been associated with acquired vitelliform lesions (Figure 2A), pseudoxanthoma elasticum, and Sorsby’s fundus dystrophy.3 Additionally, RPD need to be differentiated from similar yellowish fleck-like deposits at the macula such as other types of drusen, Stargardt’s disease, retinitis punctata albescens and fundus albipunctatus. Differentiating between these lesions can be difficult using CFP alone (Figures 2B-D), so again, we recommend using other imaging modalities as well to supplement the diagnosis.
Q: Would you recommend use of nutritional supplements for patients with RPD, even if they only have early or no AMD?
A: No. There is currently no evidence available that confirms nutritional supplements help with RPD lesions. The AREDS formula has only been proven to be effective in reducing the risk of progression to neovascular AMD in eyes with at least intermediate AMD.16
Thus, the best management for RPD is to manage the underlying condition and in the case of AMD, to be aware that there is increased risk of progression to late AMD2 and greater loss of functional vision17 when compared to conventional drusen. It is interesting to note that the AREDS studies classified AMD based off fundus photos, and thus RPD were not clearly distinguished as a unique entity from conventional drusen.16
For further controversy around the use of AREDS type supplements, see ‘bonus question.’
BONUS Q: Should patients on AREDS-type supplements be genetically tested?
A: Time will tell. Pharmacogenetic testing for AREDS supplementation has the potential to become a lot more prevalent in the future, although clinical trials are still underway and the implementation of necessary supportive resources is ongoing.
In a recent statistically-robust study regarding pharmacogenetic testing with AREDS supplementation for AMD, it was identified that: ‘individuals with high CFH and no ARMS2 risk alleles and taking the AREDS formulation had increased progression to NV (neovascularisation) compared to placebo. Those with low CFH risk and high ARMS2 risk had decreased progression risk.’18
The risk for progression to NV in the former genotype group taking AREDS supplementation was almost 300 per cent, versus just 50 per cent in the latter group.
Of note, this study confirmed previous reports that AREDS supplementation is only effective in reducing risk of progression to neovascular AMD, and not central geographic atrophy.16
If the individual results of taking supplementation are so variable, then why isn’t pharmacogenetic testing more prevalent? On the one hand, as clinicians, we should ensure that we are not harming the patient by suggesting use of the AREDS supplementation.
A recent study has also shown that a majority of participants were interested in undergoing AMD genetic testing regardless of having no signs or symptoms of AMD, as they had a family history of AMD or another genetic disorder. Results of testing being relayed to participants also subsequently led to modified behaviours to reduce the risk of AMD.19
However, on the other hand: there is the possibility of inducing anxiety and financial burden; concerns regarding the security and privacy of health data may arise, particularly if tests are available online and not properly regulated; genetic typing may lead to discrimination (by affecting eligibility for particular health insurance policies). Also: clinicians will need to be trained in interpreting and relaying all manner of results and management plans to patients.
Overall, while the evidence for pharmacogenetic testing for AREDS supplementation appears promising thus far, further trials are needed to (1) validate results particularly in different cohorts, and (2) ensure proper resources are in place before the implementation of routine pharmacogenetic testing for AMD patients.
Arnold JJF, Sarks SHF, Killingsworth MC et al. Reticular pseudodrusen: A Risk Factor in Age-Related Maculopathy. Retina 1995; 15: 183–191.
Boddu S, Michele DL, Marcela M et al. Risk Factors Associated with Reticular Pseudodrusen versus Large Soft Drusen. Am J Ophthalmol 2014; 157: 985-993.e2.
Cohen SY, Dubois L, Tadayoni R et al. Prevalence of reticular pseudodrusen in age related macular degeneration with newly diagnosed choroidal neovascularisation. Br J Ophthalmol 2007; 91: 354–359.
Chan H, Cougnard-Gregoire A, Delyfer M-N et al. Multimodal Imaging of Reticular Pseudodrusen in a Population-Based Setting: The Alienor Study. InvestOphthalmol Vis Sci 2016; 57: 3058–3065.
Smith RT, Sohrab MA, Busuioc M et al. Reticular Macular Disease. Am J Ophthalmol 2009; 148: 733-743.e2.
Ueda-Arakawa N, Ooto S, Tsujikawa A et al. Sensitivity and specificity of detecting reticular pseudodrusen in multimodal imaging in Japanese patients. Retina 2013; 33: 490–497.
Schmitz-Valckenberg S, Alten F, Steinberg JS et al. Reticular drusen associated with geographic atrophy in age-related macular degeneration. Invest Ophthalmol Vis Sci 2011; 52: 5009–5015.
Zweifel SA, Spaide RF, Curcio CA et al. Reticular Pseudodrusen Are Subretinal Drusenoid Deposits. Ophthalmology 2010: 117: 303-312.e1.
Sarks J, Arnold J, Ho I-V et al. Evolution of reticular pseudodrusen. Br J Ophthalmol 2011; 95: 979–985.
Curcio CA, Messinger JD, Sloan KR et al. Subretinal drusenoid deposits in non-neovascular age-related macular degeneration: morphology, prevalence, topography, and biogenesis model. Retina Phila Pa 2013; 33: 265–276.
Bindewald A, Bird AC, Dandekar SS et al. Classification of Fundus Autofluorescence Patterns in Early Age-Related Macular Disease. Invest Ophthalmol Vis Sci 2005; 46: 3309–3314.
Smith RT, Chan JK, Busuoic M et al. Autofluorescence Characteristics of Early, Atrophic, and High-Risk Fellow Eyes in Age-Related Macular Degeneration. Invest Ophthalmol Vis Sci 2006; 47: 5495–5504.
Lee MY, Yoon J, Ham D-I. Clinical characteristics of reticular pseudodrusen in Korean patients. Am J Ophthalmol 2012; 153: 530–535.
Saksens NTM, Fleckenstein M, Schmitz-Valckenberg S et al. Macular dystrophies mimicking age-related macular degeneration. Prog Retin Eye Res 2014; 39: 23–57.
Chew EY, Clemons TE, Agron E et al. Long-Term Effects of Vitamins C, E, Beta-Carotene and Zinc on Age-Related Macular Degeneration. AREDS Report No. 35. Ophthalmology 2013; 120: 1604-1611.e4.
Querques G, Massamba N, Srour M et al. Impact of reticular pseudodrusen on macular function. Retina Phila Pa 2014; 34: 321–329.
Vavvas DG, Small KW, Awh CC et al. CFH and ARMS2 genetic risk determines progression to neovascular age-related macular degeneration after antioxidant and zinc supplementation. Proc Natl Acad Sci USA 2018; 115: E696–E704.
McCarty CA, Fuchs MJ, Lamb A et al. How Do Patients Respond to Genetic Testing for Age-related Macular Degeneration? Optom Vis Sci 2018; 95: 166–170.
Acknowledgements The authors thank Dr Lisa Nivison-Smith for reviewing this article.
Q & A: Dry eye disease
DED: causes, symptoms and treatment options
Working with the Institute of Excellence, Pharma’s Q&A issue presents some of the most frequently-asked and relevant questions submitted by members on the ‘Taking the dryness out of dry eye webcast,’ answered here by Dr Maria Markoulli.
Maria Markoulli PhD MOptom GradCertOcTher FBCLA FAAO
Department of Optometry and Vision Science, UNSW
Q: Can you talk about the osmolarity test unit and its predictability/specificity to dry eye disease (DED), as well as the cost per test?
A: Osmolarity plays a key role in the pathophysiology of dry eye disease and forms part of the 2017 Tear Film and Ocular Surface Dry Eye Workshop II (TFOS DEWS II) diagnostic criteria. According to TFOS DEWS II, people with dry eye disease show more variability in their osmolarity measurements than their non-dry eye counterparts, and this is considered diagnostic.
The current guidelines include a difference of ≥ 8 mOsm/L between eyes, or a measurement of ≥ 308 mOsm/L for mild to moderate dry eye and ≥ 316 mOsm/L for moderate to severe dry eye.1
One challenge with the use of osmolarity has been the reported variability, for example, in people with Sjögren Syndrome and blepharitis, potentially complicating clinical interpretation.2 In a group of healthy controls, a clinically-relevant difference of 34 mOsm/L was found.2
What this means is: when a single tear osmolarity measurement is taken, such as before and after treatment, the measurement error and the variability between visits needs to be taken into account before considering the change with treatment to be clinically-relevant. This variability also means that a single measurement is not enough to distinguish between those with and those without dry eye. This large variability could explain the reported lack of association between tear osmolarity and clinical signs and symptoms.3
There are currently two devices on the market for the measurement of osmolarity: TearLab (TearLab Cooperation, California, US) and the iPen (iMedPharma, Quebec City, Canada). The TearLab equipment can be purchased outright or leased for a more affordable option. The iPen is a portable device and can also be purchased. Clinicians can contact the companies directly for a quote.
Q: Does chemotherapy or radiation therapy cause DED?
A: The antineoplastic mechanisms of chemotherapy can lead to undesirable systemic and ocular side effects resulting from cytotoxicity, inflammation and neurotoxicity.4
The ocular surface is particularly susceptible to toxicity with reported conditions including meibomian gland dysfunction, epiphora, dry eye, conjunctivitis, keratitis and ocular discomfort.4 An important factor to also consider is the interaction of ocular therapeutics with concurrent anticancer drugs. For example, oral dexamethasone can potentially decrease the concentration of anti-cancer drugs, as can certain antibiotics such as clarithromycin, and oral antifungals such as fluconazole.4
There have also been reports about radiotherapy impacting the ocular surface. One study has reported that periocular radiotherapy contributes to tear film instability as a result of meibomian gland damage.5
Q: Do we know why ‘screen time’ makes meibomian gland dysfunction (MGD) symptoms worse? Is it just from evaporative dry eye?
A: Two main theories exist – first: screen time results in a reduced blink rate,6 or a greater number of partial, rather than complete, blinks,7 and that this, in turn, impacts on the spread of the tear film, resulting in corneal desiccation.
Second: the decreased blink rate means that there is less expression of meibum, since meibum is largely expelled onto the lid margin with each blink due to the action by the muscle of Riolan within the lids.
In a study by Wang et al.,8 incomplete blinking was associated with a two-fold increased risk of dry eye disease. Hence, it is important to remind our patients about ‘blink hygiene,’ particularly when using their devices.
Q: Do you use a numbing agent prior to gland expression? And how do you know when to stop expressing each gland?
A: I use the Blephasteam for 10 minutes to heat up the lids to facilitate expression, and then instil a drop of anaesthetic into each eye.
I follow that up with a cotton bud soaked in anaesthetic that I use to run along the meibomian gland orifices to loosen up any keratinised material obstructing the orifices.
I then use lissamine green to delineate Marx’s line and debride along the meibomian gland orifices with a golf spud. Finally, I use forceps to express the glands, typically making two-to-three passes. I will often instil a corticosteroid post-expression and advise patients that they may experience some redness and discomfort post-procedure.
Q: What is the most popular/recommended heat therapy method used in retail optometry practices for in-room meibomian gland expression?
A: The Blephasteam is quite straight forward to use. Otherwise, use any heat pack like the Bruder Moist Heat Eye Compress, which is washable, or the EyeEco Derm mask, which has disposable liners.
Q: Are there any studies showing that dry eye treatment slows MG drop out? And how do you manage MG drop out?
A: Not many studies have looked at this. In a retrospective review of patients who have undergone intense pulsed light, an improvement in meibomian gland dropout was noted at three months in people with mild-to-moderate gland atrophy.9
A recent Cochrane review, however, showed that there is a current scarcity of evidence that this form of treatment has any effect on meibomian gland dropout.10 This suggests that we need more randomised, controlled, clinical studies to be conducted that include meibomian gland dropout as an endpoint.
Q: Which steroid is your drug of choice for DED?
A: The two main steroids of choice would be either Flarex (fluromethalone acetate) or FML (fluoromethalone alcohol). In the case where preserved drops are not an option, I opt for preservative-free prednisolone sodium phosphate 0.5% minims.
Wolffsohn JS, Arita R, Chalmers R et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf 2017; 15: 539-574.
Bunya VY, Fuerst NM, Pistilli M et al. Variability of Tear Osmolarity in Patients With Dry Eye. JAMA Ophthalmology 2015; 133: 662-667.
Tashbayev B, Utheim TP, Utheim Ø A et al. Utility of Tear Osmolarity Measurement in Diagnosis of Dry Eye Disease. Sci Rep 2020; 10: 5542.
Chiang JC, Zahari I, Markoulli M et al. The impact of anticancer drugs on the ocular surface. Ocul Surf 2020.
Woo YJ, Ko J, Ji YW et al. Meibomian Gland Dysfunction Associated With Periocular Radiotherapy. Cornea 2017; 36: 1486-1491.
Patel S, Henderson R, Bradley L et al. Effect of visual display unit use on blink rate and tear stability. Optom Vis Sci 1991; 68: 888-892.
Argilés M, Cardona G, Pérez-Cabré E et al. Blink Rate and Incomplete Blinks in Six Different Controlled Hard-Copy and Electronic Reading Conditions. Invest Ophthalmol Vis Sci 2015; 56: 6679-6685.
Wang MTM, Tien L, Han A et al. Impact of blinking on ocular surface and tear film parameters. Ocul Surf 2018; 16: 424-429.
Yurttaser Ocak S, Karakus S, Ocak OB et al. Intense pulse light therapy treatment for refractory dry eye disease due to meibomian gland dysfunction. Int Ophthalmol 2020; 40: 1135-1141.
Cote S, Zhang AC, Ahmadzai V et al. Intense pulsed light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev 2020; 3: Cd013559.
Q & A: Glaucoma
Progression analysis and the evidence on intervention
Working in tandem with the Institute of Excellence, the Q&A issue presents some of the most frequently-asked and relevant questions submitted by members on the ‘Glaucoma webcast,’ answered here by Dr Jack Phu.
Jack Phu BOptom (Hons) BSc MPH PhD FAAO Diplomate (Glaucoma)
Lead Clinician (Glaucoma)
Centre for Eye Health
Associate Lecturer School of Optometry and Vision Science, UNSW
Centre for Eye Health and the School of Optometry and Vision Science UNSW
Q: What is the minimum time required between optical coherence tomography (OCT) scans to detect progression? For example, if you take a baseline for a patient with a suspicious optic nerve head (ONH), in the interest of minimising patient costs, how long should you wait before taking a repeat OCT to detect change?
A: Currently, OCT devices do not account for age-related change when performing the change analysis.
When a change is identified as significant, it only signifies that there is a significant difference to 0. In other words, it’s a statistical test, but not a clinical indicator.
This is different to visual field testing, where indices like the mean deviation score is corrected for age. Furthermore, some progression analyses include confidence intervals or error bars for the slope, which accounts for the variability in the measurement. It is essential for clinicians to account for test-retest variability–which may differ across instruments–to make accurate judgements on progression.
Studies examining visual field changes typically use an interval of two years for progression analysis. Fortunately, disease progression in glaucoma tends to occur slowly, and significant vision loss is unlikely to occur within two years.1
This is something for the clinician to bear in mind in terms of the urgency at which progression needs to be detected.
As a rule-of-thumb then, a clinician following the manufacturer’s recommendations should use a minimum of five test results over a period of two years (assuming two baseline scans).
It is important to remember that follow-up should occur in the interim, with repeat testing indicated and titrated based on suspicious findings, such as patients in whom there are other risk factors such as pseudoexfoliation. In the case of glaucoma, signs such as intraocular pressure fluctuations or elevations, or disc haemorrhages should signal the need to reassess.
Q: Is race/ethnicity a variable in OCT analysis and if yes, what is the basis for this?
A: Race and ethnicity have been comprehensively demonstrated to affect relevant ocular biometric parameters and may play roles in the epidemiology of disease.2 The basis of this is biological.
For example, the work of Girkin et al.3 showed that European patients have smaller optic disc areas compared to other races, Indian patients have smaller rim area, Indian and Hispanic patients have thicker global retinal nerve fibre layer measurements, and African patients have thinner inner retinal thickness at the macula.
These findings are largely corroborated by Knight et al.,4 who highlighted that people of African descent have large disc size, cup-disc ratio and cup volume compared to people of other races.
A question remains regarding individuals of mixed race. This has not been studied in the literature.
While race and ethnicity have been acknowledged to be important in the interpretation of OCT results, many instruments do not have normative databases of sufficient ethnic diversity to perform race-specific analyses. Indeed, there are comments that other forms of biometric diversity such as refractive error5 should be considered.
Q: What advice do you generally tell patients regarding diet, supplements and lifestyle?
A: Glaucoma is a multifactorial disease and risk factors–individually or in combination–contribute to the overall course of the disease in a complex manner. There are no robust evidence-based guidelines to support significant modifications to diet, supplementation and lifestyle specifically for glaucoma risk.
Reports in the literature are largely limited to observational studies, far from the expected standard of a randomised clinical trial. Clinicians should remain wary and sceptical, as observational studies have a high risk of biases including selection bias. See Al Owaifeer and Al Taisan for a review.6
The clinician should bear in mind though that this kind of advice would be specific to the individual and their own circumstances.
Furthermore, there is evidence to show that effects from any of these interventions are likely transient (for example, intraocular pressure reductions lasting in the order of minutes) and are unlikely to significantly affect the course of a chronic disease.7 Thus, no specific interventions are currently supported by the literature.8
Q: Is there any association between the gut microbiome and glaucoma?
A: The link between gut microbiome and glaucoma has been hypothesised to arise from the microbiota-gut-retina axis:9 the resultant autoantibodies and auto-reactive T cells lead to autoimmunity and hence damage to the optic nerve.
Analogous neurodegenerative diseases such as Alzheimer’s disease and Parkinson’s disease have also been linked to gut microbiome. As evidence is still emerging, it may be better to regard gut microbiome as an emerging risk factor for glaucoma, in the same manner as other systemic vascular or ischaemic disease.
Heijl A, Bengtsson B, Hyman L et al. Natural history of open-angle glaucoma. Ophthalmology 2009; 116: 2271-2276.
Tham YC, Li X, Wong TY et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 2014; 121: 2081-2090.
Girkin CA, McGwin G, Jr., Sinai MJ et al. Variation in optic nerve and macular structure with age and race with spectral-domain optical coherence tomography. Ophthalmology 2011; 118: 2403-2408.
Knight OJ, Girkin CA, Budenz DL et al. Effect of race, age, and axial length on optic nerve head parameters and retinal nerve fiber layer thickness measured by Cirrus HD-OCT. Arch Ophthalmol 2012; 130: 312-318.
Seol BR, Kim DM, Park KH et al. Assessment of Optical Coherence Tomography Color Probability Codes in Myopic Glaucoma Eyes After Applying a Myopic Normative Database. Am J Ophthalmol 2017; 183: 147-55.
Al Owaifeer AM, Al Taisan AA. The Role of Diet in Glaucoma: A Review of the Current Evidence. Ophthalmol Ther 2018; 7: 19-31.
Risner D, Ehrlich R, Kheradiya NS, et al. Effects of exercise on intraocular pressure and ocular blood flow: a review. J Glaucoma 2009; 18: 429-436.
Hecht I, Achiron A, Man V et al. Modifiable factors in the management of glaucoma: a systematic review of current evidence. Graefes Arch Clin Exp Ophthalmol 2017; 255: 789-796.
Chaiwiang N, Poyomtip T. Microbial dysbiosis and microbiota-gut-retina axis: The lesson from brain neurodegenerative diseases to primary open-angle glaucoma pathogenesis of autoimmunity. Acta Microbiol ImmunolHung 2019; 66: 541-558.
June 2020
Chair-side Reference: Screening Ocular Toxicity of Selected Drugs
A reference guide describing the major potential ocular side effects related to selected systemic drugs, including signs and symptoms, recommendations on the workup and ongoing follow-up intervals in an optometric setting.
Guest editor Roman Serebrianik asks Mitchell D Anjou the question: ‘Why should optometrists ask their patients if they are Aboriginal or Torres Strait Islander origin?
Mitchell D Anjou AM BScOptom MScOptom FACO
Academic Specialist, Indigenous Eye Health group
Senior Research Fellow and Deputy Director
The University of Melbourne
Roman Serebrianik BOptom PGDipAdvClinOptom PGCertOcTher FACO
Senior Policy Advisor
Vision 2020 Australia
Guest Clinical Editor of Pharma
Many optometrists are aware that eye and vision problems are the most common long-term health conditions experienced by Aboriginal and Torres Strait Islander people.
Pharma’s Guest Clinical Editor Roman Serebrianik recently conducted an interview with Mitchell Anjou from The University of Melbourne’s Indigenous Eye Health (IEH). Established in 2008, IEH guides government policy to ‘close the gap’ between the health outcomes of Aboriginal and Torres Strait Islanders and other Australians.
RS: What are the most pressing problems for the Indigenous population?
MA: The immediate and current challenge for Indigenous eye care in Australia is to provide support and care for communities through the COVID-19 pandemic.
Most remote communities have effectively isolated for visitors and visiting services and the impact here is twofold: a lack of care and a consequent backlog of care.
The backlog presents challenges such as distribution of the finite resource that supports eye care (Australian Government programs including the Visiting Optometrists Scheme (VOS), Rural Health Outreach Fund (RHOF), the Medical Outreach Indigenous Chronic Disease Program (MOICDP) and Eye and Ear Surgical Support Services (EESSS) do not readily allow additional services, nor are there the physical and workforce resources available to provide this).
Urgent and emergency care will likely be compromised during the pandemic and regular care, including the delivery of diabetic retinopathy intravitreal injections will be impacted.
A further concern is that this period may allow the gap to broaden unless Aboriginal and Torres Strait Islander eye care is prioritised in the post COVID-19 period.
Beyond COVID-19, the focus is further system enhancement, reform and growth as characterised in Vision 2020 Australia’s ‘Strong Eyes, Strong Communities’ plan.
RS: Could you describe the work of the Indigenous Eye Health Unit (IEH)?
MA: Indigenous Eye Health at The University of Melbourne was established by Professor Hugh Taylor in 2008 with a singular purpose to work towards ensuring that the gap for vision was closed–that is: that there would be no population-level difference in rates of unnecessary blindness and vision loss between Aboriginal and Torres Strait Islander and other Australians.
The strategies used in the work have included: national surveys to measure blindness and vision loss rates and causes; analysis of available national data on eye care services and their use; case study consideration of service models and their various successes and shortfalls; extensive community and sector consultation on the barriers to access and utilise care; and the development of solutions to these barriers.
This work was consolidated in 2012 as ‘The Roadmap to Close the Gap for Vision’ and the group works to implement the Roadmap health systems reforms.
A key element of the Roadmap has been the elimination of trachoma in Australia.
We characterise our work as offering technical advice and support for those implementing the systems changes recommended by the Roadmap that will lead to the gap for vision being closed. Within the academy we are considered ‘translational researchers.’
RS: What’s the history behind ‘Close the Gap?’ and more specifically, the ‘Close the Gap: Vision’ programs?
MA: The ‘closing the gap’ campaign has origins back to 2008 where Australian governments (national, state and territory) agreed to work together to deliver better health, education and employment outcomes for Aboriginal and Torres Strait Islander people, and to eliminate the gaps between Indigenous and non-Indigenous Australians.
Our work has been more closely aligned to the ‘close the gap’ campaign which is Indigenous-led and has Indigenous health equality by 2030 as the goal.
The Close the Gap for Vision work has been underpinned by the Roadmap and has a specific focus on eliminating the inequity between Aboriginal and Torres Strait Islander blindness and vision loss to other Australians.
RS: What’s working?
MA: Optometrists know how to examine eyes and so, from my perspective, there has never been a clinical deficiency in our care for Indigenous Australians.
The issues have been access to and availability of services, the appropriateness of services and the cultural safety of care offered.
I have been very keen to encourage optometrists to seek out patients in their communities who may not readily access care and to ensure all people in their communities are not unnecessarily suffering vision loss and eye disease.
Working from Aboriginal community-controlled health settings, optometrists provide additional outreach and remote and regional services. They contribute to regional collaboratives providing eye care, improving and offering subsidised spectacles services. Optometrists also support primary care services to identify and assist those with eye problems in all areas. And our work has made a significant difference.
RS: What can optometrists do to help?
MA: Optometry is key to improved vision and eye health for Aboriginal and Torres Strait Islander Australians.
Good vision is critical to health and well-being. Indeed, analysis in 2011 estimated that vision loss represented some 11 per cent of the Aboriginal health burden.
Optometry, working with and within Aboriginal community-controlled health settings, can demonstrate how to successfully link primary care and specialist services—and this model is applicable in other areas of health.
Improving vision and eye health also illustrates improved health achievement and demonstrates immediate advantage and success.
However, our goal is that this work is community-driven and led and that is the important work of the next few years.
Optometrists can also contribute to visiting work for communities that do not have resident practitioners.There are a number of agencies and private practices that support these opportunities.
My wish is that optometrists look at their own communities first and check whether they are providing care to the Aboriginal people in their area – and ensuring that the care is culturally safe.
RS: Why should optometrists ask their patients if they are Aboriginal or Torres Strait Islander origin?
MA: The ‘Have you Asked the Question‘ resource is an important initiative that we hope encourages all eye care practitioners to consider the services and care that they provide to Aboriginal and Torres Strait Islander people.
We have been pleased that other health providers, including GPs, are displaying the resource.
For me, creating discussions in optometry practices about Indigenous eye care might be challenging but can only be positive and may result in friendlier, more-knowledgeable and safer places for Aboriginal people to attend for care.
Practices and practice staff who are comfortable ‘asking the question’ are demonstrating some cultural competence. When patients choose to identify, the practitioner is then in a position to ensure that approaches to care and support for care can be accessed for them.
RS: What’s next for the IEH and you?
MA: ‘Beyond 2020’ presents a number of opportunities for IEH and we continue to consider and work through these.
The ‘Roadmap to Close the Gap for Vision’ has made great strides and hopefully the upcoming second National Eye Health Survey will confirm more progress, and indeed that the gap is effectively closed.
Vision 2020 Australia, on behalf of the eye care sector, has developed the ‘Strong Eyes, Strong Communities plan for 2019-2024’ and IEH is participating in the implementation and delivery of this plan.
Probably the most exciting advancement here is increasing community leadership and control of eye care.
The Australian Government has also identified the elimination of avoidable blindness and vision loss for Aboriginal and Torres Strait Islander people as a goal for 2025—there remains work to do.
IEH identifies other areas of Aboriginal and Torres Strait Islander health where an approach like that undertaken in eye care could be applied. We are considering how best to employ the lessons we’ve learned in eye care to other areas of Indigenous health.
For me, I am happy to contribute where I am useful and wanted. I have enjoyed a wonderful professional life in optometry and I hope that my experiences and skills can be applied to support future challenges in public health, health equity and eye care.todate.com/contents/diagnosis-of-hyperthyroidism
A unique case: An original case report by Optometry Australia member Laura Carson
Idiopathic, thyroid eye disease or myopia-associated esotropia syndrome?
Laura E Carson BVisSci Moptom
Canterbury Eyecare, Canterbury VIC
A 23-year-old female myopic female presented with symptoms of intermittent diplopia, worse when wearing glasses than soft contact lenses (CLs). Visual acuity (VA) with her monthly replacement CLs were R 6/7.5 and L 6/6. Motilities and pupil reactions were normal.
Cover test while wearing CLs found esophoria at distance and near, with a magnitude of 9 prism dioptres (PD) and 19 PD, respectively. Spectacle refraction results were R -5.00/-1.25×100 VA 6/6- and L -5.00/-0.75×65 VA 6/6- with 6 base out (BO) PD split to neutralise intermittent esotropia. Stereopsis was 200 seconds of arc. Fundus examination was unremarkable (Figure 1).
She was diagnosed with transiently decompensating esophoria and a review for cycloplegic refraction was scheduled to determine if the underlying cause was accommodative. In the meantime, she was prescribed monthly replacement high add multifocal CLs, aiming to control the esophoria.
Review 1
The patient was reviewed two weeks later. She reported general improvement with the change to her CL prescription but was still closing one eye to eliminate occasional diplopia. Cycloplegic refraction results were consistent with previous findings and confirmed the need for prism correction. She was prescribed prescription glasses with 6 BO prism divided and a separate pair of plano glasses with fresnel prism (10 BO) for over the top of her CL’s, to be used when driving. Thankfully this combination was satisfactory until she re-attended 12 months later for an update to her glasses and CL prescription, maintaining the prism corrections with both.
Review 2
Another 12 months later, the patient attended with symptoms of almost constant diplopia in her CL’s and felt unable to wear them for long periods of time. Cover testing found a 18 PD esophoric deviation at distance when wearing CL’s. Her existing 10 BO fresnel glasses only just controlled her diplopia. In glasses she was esotropic and exhibiting suppression at distance; cover test measured a total of 10 BO to neutralise the esotropia. Additionally, distance base in fusional reserves were limited with break at 2 PD, resolution at 1 PD. Aside from increasing the prism correction in her glasses, alternative management such as modifying her CLs and referral for an opinion on strabismus surgery was discussed.
Referral
After unsuccessful trials of alternative contact lens options, she was referred to a strabismus specialist. The ophthalmologist confirmed the measurements of her esophoria to decompensating esotropia and limited stereo acuity. Interestingly, considering her level of myopia, axial lengths were found to be R 24.11 and L 23.94 mm. She was also found to have R superior oblique underaction and associated non commutative versions (Figure 2) indicating possible abnormal lateral rectus muscle pulley anatomy. Differential diagnoses therefore became one of the myopia-associated esotropia syndromes, such as heavy eye syndrome or knobby eye syndrome.
She was sent for magnetic resonance imaging (MRI) to investigate further. The consultant radiologist reported that the MRI (Figure 3) showed ‘somewhat prominent’ extraocular muscles but still ‘symmetrical in appearance and position.’ They hypothesised Graves’ disease, introducing a new differential diagnosis, however, blood tests did not confirm any active thyroid levels. The patient no longer wanted to be reliant on any level of prism correction so decided to proceed with surgical intervention–strabismus surgery.
One week post-surgery the findings were promising. VA’s were R 6/7.6 and L 6/7.6 with glasses (a pair was made up without prism prior to surgery). She had near esotropia but distance orthophoria as well as an improvement in her stereopsis results, achieving 100 sec of arc.
Two weeks later, she attended with symptoms of worsening vision; VA with existing glasses was R 6/12+ and L 6/9.5= and refraction found a myopic shift of -0.75 in each eye, enabling a best corrected VA of R&L 6/6-. At her scheduled review with the ophthalmologist, her myopic shift was confirmed along with findings of improved stereoacuity of 70 sec of arc. She maintained distance orthophoria, albeit still with low fusional reserves. It was hypothesised that a change in corneal topography (Figure 4A, 4B) had caused the myopic shift, however, when her pre-and post-operative topography maps were compared (Table 1) this hypothesis was found to be unlikely.
Two months after surgery, the patient was found to have a stable prescription of R -7.00 VA 6/6- and L -6.25/-0.50×10 VA 6/6- which was prescribed in spectacles. Cover test found residual esophoria of 1 PD at distance and 4 PD at near. The patient is very pleased to be relieved of prismatic correction and has returned to wearing spherical monthly replacement CLs.
It has not been possible to ascertain a final diagnosis but this case highlights the management pathway and successful outcome of strabismus surgery in a unique case of progressive esophoria.
Discussion
Potential differential diagnoses included thyroid eye disease (TED) and myopia-associated esotropia syndromes such as myopic strabismus fixus subtype heavy eye syndrome (HES) or knobby eye syndrome (KES).1
Strabismus occurs in TED when there is acute inflammation followed by fibrosis of the extraocular muscles.2 In TED, all extraocular muscles may be involved and it may be unilateral or bilateral.2 In this case, negative findings on blood tests mean that there was no active immunological stimulus, but perhaps still a potential differential diagnosis.
Myopia, at any level, may lead to ocular motility issues.1 Acquired causes of ocular motility issues in myopes may be diagnosed as myopia strabismus fixus which has the subtypes esotropia-hypotropia complex (also known as HES) and the rarer exotropia-hypotropia complex.1 Additionally, axial myopia is associated with staphylomata, which, in turn, has been associated with defects of the lateral rectus-superior rectus (LR-SR) band and inferior displacement of the lateral rectus.3
HES causes symptoms of progressive esotropia, sometimes also hypotropia.4 It is similar to another condition, sagging eye syndrome. This occurs primarily in elderly patients so was excluded as a differential diagnosis early on.4 HES has been described as a displacement of rectus muscles, in particular, the lateral rectus, possibly due to dislocation of the myopic globe or compression of the muscles by the eyeball against the orbital wall.4,6-7
Recent research using MRI technology has led to the term ‘KES,’ which has been described as a syndrome parallel to HES in patients with similar symptoms. KES and HES may both occur in myopes, but strabismus caused by KES is from the interaction of the extra ocular muscles (EOMs) and a staphyloma.7 In KES, equatorial staphylomata may affect EOM paths when there is rotational contact with the EOMs, in turn adding tension which increases on ductions.7
Staphyloma prevalence increases with axial length, however they may still be present in eyes with axial lengths below 26.5mm.8 In this case, interestingly, the patient had normal axial lengths and the absence of a posterior staphyloma on fundus examination (Figure 1) as well as an absence of equatorial staphyloma on MRI (Figure 3), therefore ruling out KES and HES as potential diagnoses.
It is possible the cause in this case was idiopathic, due to TED or perhaps caused by a subtype in the family of myopia esotropia associated syndromes yet to be defined.
Kekunnaya R, Chandrasekharan A, Sachdeva V. Management of Strabismus in Myopes. Middle East Afr J Ophthalmol 2015; 22: 298–306.
Harrad R. Management of strabismus in thyroid eye disease. Eye (Lond) 2015; 29: 234–237.
Li Y, Wei Q, Le A et al. Rectus Extraocular Muscle Paths and Staphylomata in High Myopia. Am J Ophthalmol 2019; 201: 37-45.
Tan R, Demer J. Heavy eye syndrome versus sagging eye syndrome in high myopia. J AAPOS 2015; 19: 500–506.
Rutar T, Demer J. “Heavy Eye” syndrome in the absence of high myopia: A connective tissue degeneration in elderly strabismic patients. J AAPOS 2009; 13: 36-44.
Ranka M, Steele M. Esotropia associated with high myopia. Curr Opin Ophthalmol. 2015; 26: 362-365.
Demer J. Knobby Eye Syndrome. Strabismus 2018; 26: 33-41
Ohno-Matsui K. Posterior staphyloma in pathologic myopia. RetinPhysician [serial on the internet]. 2017 Jan [cited 21 Oct 2019] Available from: https://www.retinalphysician.com/issues/2017/january-2017/posterior-staphyloma-in-pathologic-myopia 87: 389-391.
March 2020
Pregnancy and the eye
Danica J Marrelli OD, FAAO
Clinical Professor, Assistant Dean of Clinical Education University of Houston College of Optometry, USA
Ocular changes and pregnancy
It’s vital that optometrists are aware of the ocular changes associated with pregnancy, as well as the risks involved in the use of ophthalmic medications during pregnancy. The hormonal effects of pregnancy cause changes in many organ systems, including the eye. The ocular changes during pregnancy are typically transient, and may be classified as physiologic, pathologic, or modifications of pre-existing conditions.
The optometrist’s role may differ depending on the condition encountered. For benign or minor conditions, the responsibility may be to counsel and reassure or to manage the minor condition independently through complete resolution. However, some conditions may need referral to ophthalmology for further evaluation or management.
Rarely, the investigation of an ophthalmic complaint may reveal a serious life-threatening condition. In this situation, the optometrist must make the appropriate referral to the obstetrician or to the emergency department for urgent care.
Physiologic changes
Typically, physiologic changes associated with pregnancy are transient and seldom pose a significant risk to long-term vision. Physiologic changes during pregnancy most commonly affect eyelids, cornea and intraocular pressure (IOP). Hyperpigmentation of sun-exposed skin (known as ‘chloasma’ or ‘melasma’) may affect the eyelids or periorbital skin. The condition is self-limited, and often resolves post-partum.1 Because the skin change is benign, no treatment or referral is necessary.
Corneal changes during pregnancy have been well-documented and include an increase in thickness and curvature, which may result in changes in refractive error. Historically, it has been advised to wait several weeks post-partum to prescribe spectacle or contact lenses.2 However, there are few studies that systematically examine refractive changes in pregnancy. Pizzarello found that pregnant women who complained of vision changes had myopic shifts of nearly one dioptre, all of which returned to near pre-pregnancy levels.3 Similar findings were observed in a study of pregnant Nigerian women, which found the shifts occur most frequently during the third trimester.4
Pregnancy has also been identified as a potential risk factor for post-LASIK corneal ectasia.5 For this reason, it is recommended to postpone pregnancy for one year following laser refractive surgery and to postpone refractive surgery for three to six months following pregnancy and lactation, and only once the refraction has stabilised.
Contact lens intolerance has been reported in 25–30 per cent of pregnant women. Corneal sensitivity is reported to decrease during pregnancy, so contact lens intolerance may be related to a decrease in tear production, or other pregnancy-related changes in the cornea, conjunctiva or lids.6 The appearance of transient Krukenberg spindles without other signs of pigment dispersion syndrome have been reported.1
Intraocular pressure decreases by approximately 10–15 per cent during the pregnancy, most notably during the second half of pregnancy, and there is a decrease in diurnal fluctuation of IOP. No decrease in aqueous production has been demonstrated, so the decrease in IOP is likely due to increased trabecular outflow and/or reduced episcleral venous pressure. IOP returns to pre-pregnancy levels approximately two months post-partum.7 The effect of pregnancy on pre-existing glaucoma has not been well studied, nor have the risks of glaucoma management been fully established.
Pathologic changes
Two key pathologic changes associated with pregnancy of which primary eye care professionals should be aware include: central serous chorioretinopathy and pregnancy-induced hypertension.
CSC
Central serous chorioretinopathy (CSC) is a spontaneous, localised serous detachment of the neurosensory retina from the underlying retinal pigment epithelium. It is typically self-limited, but may be recurrent or chronic. It is much more common in men than women, and pregnancy is a well-documented risk factor for the development of CSC. It is thought that increased levels of endogenous corticosteroids during pregnancy may be the reason for the increased incidence during pregnancy. Other risk factors include smoking, Helicobacter pylori infection and obstructive sleep apnoea. Patients with a history of CSC prior to pregnancy should be advised that it may recur during pregnancy; however, there are no recommendations for additional examinations during pregnancy.
CSC in pregnancy is most common in the third trimester, and is more likely to have yellow subretinal fibrin deposits compared to CSC in men and non-pregnant women.8 It typically resolves by one to two months post-partum, but has been reported to recur in subsequent pregnancies.1,9
Optical coherence tomography (OCT) is a non-invasive diagnostic tool that allows for diagnosis of CSC without the need for invasive intravenous fluorescein angiography. CSC during pregnancy is not associated with fetal risks.
PIH
Pregnancy-induced hypertension (PIH) includes pre-eclampsia and eclampsia. Pre-eclampsia includes hypertension and proteinuria. Eclampsia is diagnosed when a pre-eclampsia patient develops seizures. Eclampsia is a life-threatening emergency, and immediate attention must be given. Both pre-eclampsia and eclampsia have been reported to cause vision disturbances including blur, photopsia and visual field defects.
Clinically, the most common ocular finding of PIH is localised or generalised constriction of the retinal arterioles. Other findings of hypertensive retinopathy (intraretinal haemorrhages, cotton wool spots) may also be seen.
All vision changes associated with PIH should be taken very seriously, as they may indicate an impending seizure and require immediate care. The appropriate referral of such a patient is an immediate referral to the obstetrician rather than to a retinal specialist.10 Severe vision loss is rare but possible in PIH. Serous exudative retinal detachments as well as cortical blindness have been reported. Fortunately, both conditions tend to resolve days to weeks following delivery.
Pre-existing conditions
Pregnancy is an independent risk factor for worsening of diabetic retinopathy. Pre-existing diabetes is present in 1 in 167 pregnancies in Australia.11 The more severe the level of retinopathy at conception, the more likely there will be progression during pregnancy.
Other risk factors for progression of retinopathy include duration of diabetes and poor pre-pregnancy glucose control. Gestational diabetes is not associated with diabetic retinopathy. While regression of retinopathy is common in the post-partum period, some women will continue to experience worsening for up to one year following delivery. Therefore, careful monitoring of diabetic patients during the first year post-partum is important.10,11 Examination recommendations vary depending on the organisation, but there are some common guidelines.
A comprehensive eye examination is recommended in the first trimester for all pregnant women with pre-existing diabetes. Depending on the level of retinopathy found during the first trimester, additional examinations are recommended later in the pregnancy. For example, the American Academy of Ophthalmology recommends an eye exam for pregnant patients with diabetes every three to 12 months if no retinopathy or mild nonproliferative retinopathy (NPDR) is present, and an exam every one to three months if the retinopathy is severe NPDR or worse.12
Pan-retinal photocoagulation (PRP) is safe during pregnancy. Typically reserved for patients with proliferative disease, several guidelines recommend PRP earlier in pregnant patients (at the level of severe non-proliferative retinopathy).10
Treatment of diabetic macular oedema (DME) in pregnant women is more controversial. Data is lacking as to the natural history of DME during pregnancy, and the American Academy of Ophthlamology guidelines recommend delaying focal laser treatment in pregnant patients.
Anti-VEGF injections have emerged as a more recent treatment option for DME. Their use during pregnancy is controversial, however, as they may cause systemic side effects to the mother and foetus, including loss of pregnancy.12 Several case reports have been published in which spontaneous miscarriage occurred shortly after intravitreal anti-VEGF injections. While causation cannot be determined, Polizzi and Mahajan recommend that anti-VEGF be utilised only when the benefit to the woman justifies the risk to the foetus.13
The optometrist plays an important role in the care of the diabetic patient. Unless the patient presents with retinopathy requiring treatment, the optometrist can provide the examination and testing such as fundus photography and optical coherence tomography (OCT), and can make the appropriate recommendations regarding follow-up care. If the retinopathy requires treatment, a referral to an ophthalmologist or retinal specialist is appropriate. In all cases, whether or not treatment is needed, the optometrist has an obligation to communicate the examination findings and recommendations with the patient’s general practitioner and obstetrician.
Use of ophthalmic medications during pregnancy and lactation
Caution should be used when administering or prescribing medication to a pregnant woman. Topical medications may be absorbed through the nasolacrimal mucosa and may pass through the placenta or be excreted in breast milk, creating a potential risk to the foetus or neonate. Limited data is available on the safety of medication use in pregnancy, particularly the use of topical medications. A review by Chung suggested that the topical ophthalmic use of medications during pregnancy presents very low risk of harm due to the small amounts of medication absorbed.14 However, general guidelines for use of ophthalmic medications during pregnancy and lactation include: avoid medications if possible during the first trimester; avoid unnecessary drugs throughout pregnancy; use the smallest dose and shortest duration necessary to achieve the desired therapeutic effect; and use digital nasolacrimal occlusion or gentle eyelid closure for several minutes following instillation to reduce systemic absorption. Consulting with the patient’s obstetrician or pharmacist about the utilisation of pharmaceutical agents is appropriate in some situations. Finally, the patient should be informed about the medication choices and the information (or lack thereof) related to the safety of the proposed treatment. Information is available from a variety of sources. The drug package insert may contain information related to pregnancy and lactation, although many drugs have not been well studied. Texts such as Drugs in Pregnancy and Lactation (Brigg, et al) provide information on many medications. Websites such as mothertobaby.org also provide referenced, scientific evidence on a variety of medications. However, ophthalmic (topical) medications are often overlooked in such references.
Diagnostic agents
Topical anesthetics and sodium fluorescein dye used in a routine ophthalmic examination are considered safe during pregnancy. Mydriatic and cycloplegic agents are all assigned Category C (animal reproductive studies have shown an adverse effect on the foetus, but there are no adequate human studies), but their topical ophthalmic use has not been studied extensively. Generally, dilated eye exams are deferred until post-partum. While non-mydriatic wide-field photography does not replace pupillary dilation, it may be appropriate in lieu of dilation in routine cases. However, in situations in which dilation is important for diagnosis, such as a patient with a complaint of photopsia or a patient with pre-existing diabetes, the benefit of the dilation outweighs the risks, and dilation should be performed. Chawla et al reported that the use of dilating drops during pregnancy is safe.15
Anti-infective agents
Consideration must be given to the risk and benefit of treating an ocular infection during pregnancy. While unnecessary medications should be avoided, a pregnant patient should not be required to suffer needlessly.
Non-pharmacologic measures such as warm compresses and lid scrubs for blepharitis, or saline rinses for mild bacterial conjunctivitis, may be considered in lieu of drug therapy. However, a bacterial keratitis presents significant risk of permanent vision loss if not treated promptly. The optometrist should not hesitate to treat painful and/or sight-threatening infections with medication.
Topical anti-bacterial agents in Category B (presumed safe) include azithromycin, erythromycin and tobramycin. Topical fluoroquinolones are all labeled Category C (unknown safety) except for besifloxacin, which reports no available human data. Given a variety of available Category B topical medications, it would be prudent to avoid the fluoroquinolones in the treatment of conjunctivitis. However, given their efficacy in treating bacterial keratitis, the benefit of their use in a corneal ulcer likely outweighs any small risk involved.
Systemic antibiotics may be needed in the case of a soft tissue (lid) infection. Penicillins and cephalosporins, commonly utilised in the management of internal hordeolum or preseptal cellulitis, are considered safe during pregnancy. Likewise, erythromycin and azithromycin are considered safe to use. Tetracycline and its derivatives should be avoided in both pregnant and lactating women due to the possibility of bone and teeth abnormalities in the foetus/infant.
Oral antivirals acyclovir, valacyclovir, and famciclovir are Category B medications and are generally considered safe during pregnancy. Given the potential complications of untreated herpetic infections, the benefit outweighs the risks of antiviral therapy.
Anti-inflammatory and allergy agents
Most topical antihistamine agents are designated Cateory C. Despite this designation, there are no reported adverse effects from topical antihistamine agents. Limited use for symptomatic patients when non-pharmacologic intervention is insufficient in relieving symptoms, is probably safe during acute episodes of significant ocular allergy. While systemic corticosteroids are a relative contraindication during pregnancy, there are no known teratogenic effects of topical steroids.14,15 When considering the potential risks of untreated anterior uveitis, the benefits of topical steroid therapy likely outweigh the risks.
Anti-glaucoma agents
Brimonidine is the only Category B glaucoma medication. However, since brimonidine can cause severe central nervous system depression in neonates and infants, it should be discontinued prior to delivery and avoided during lactation.16 Topical beta-blockers have been associated with foetal bradycardia. However, systemic beta blockers are often used by obstetricians to treat systemic hypertension in pregnant women; as such, topical timolol, particularly in the lowest concentration used once daily, is probably safe during pregnancy. Some experts recommend discontinuing several days prior to delivery to avoid foetal bradycardia.14-15 Prostaglandin analogs are associated with premature labour or miscarriage in animal studies. Although there are case series in the literature in which pregnant women were exposed to latanoprost with no adverse pregnancy outcome, this class of medication should be avoided during pregnancy. Oral acetazolamide has been associated with teratogenic effects on the foetus. No reports of adverse effects have been reported from topical carbonic anhydrase inhibitor use.17
Because intraocular pressure is often reduced during pregnancy, it may be possible to manage glaucoma without medication or with limited medication to reduce the risk of harm to the foetus. Laser trabeculoplasty may also be an appropriate option for pregnant patients who need additional IOP lowering.
Summary
Pregnancy is responsible for many changes in the eye. Physiologic changes, while benign, may result in the pregnant patient presenting to the optometrist for care. Pathologic changes may also bring the pregnant patient in for evaluation. It is important for the optometrist to be familiar with the benign and more serious complications associated with pregnancy. In the event that medical therapy is indicated, a cautious approach is indicated to minimise potential harm to both the mother and the developing foetus.
References
Bolanca Z, Kuna K, Vukovic A et al. Chloasma—the mask of pregnancy. Coll Antropol 2008; 32: 139-141.
Nkiru Z, Obiekwe O, Lilian O et al. Visual acuity and refractive changes among pregnant women in Enugu, Southesat Nigeria. J Family Med Prim Care 2018; 7: 1037-1041.
Sharma S, Rekha W, Sharma T et al. Refractive issues in pregnancy. Aust N Z J Obstet Gynaecol 2006; 46: 186-188.
Hafezi Koller T, Derhartunian V, Seiler T.Pregnancy may trigger late onset of keratectasia after LASIK. J Refract Surg 2012; 28: 242-243.
Horven I, Gjonnaess H, Kroese A. Corneal indentation pulse and intraocular pressure in pregnancy. Arch Ophthalmol 1974; 91: 92-98.
Sunness JS, Haller JA, Fine SL. Central serous chorioretinopathy and pregnancy. Arch Ophthalmol 1993 Mar; 111 (3): 360-4
Rosenthal JM, Johnson MW. Management of retinal diseases in pregnant patients. J Ophthalmic Vis Res 2018; 13: 62-65
Schultz K, Birnbaum A, Goldstein D. Ocular disease in pregnancy. Curr Opin Ophthalmol 2005; 16: 308-314
Morrison JL, Hodgson LA, Lim LL et al. Diabetic retinopathy in pregnancy: a review. Clin Exp Ophthalmol 2016; 44: 321-334
American Academy of Ophthalmology Retina/Vitreous Panel. Preferred Practice Pattern Guidelines. Diabetic Retinopathy. San Francisco, CA: American Academy of Ophthalmology; 2017. Available at: www.aao.org/ppp
Polizzi S, Mahajan V. Intravitreal Anti-VEGF injections in pregnancy: case series and review of literature. J Ocul Pharmacol Ther 2015; 31: 605-610.
Chung C, Kwok A, Chung K. Use of ophthalmic medications during pregnancy. Hong Kong Med J 2004; 10: 191-195.
Chawla S, Chaudhary T, Aggarwal S et al. Ophthalmic considerations in pregnancy. Med J Armed Forces India 2013; 69: 278-284.
Sethi HS, Naik M, Gupta VS. Management of glaucoma in pregnancy: risks or choices, a dilemma? Int J Ophthalmol 2016; 9: 1684-1690.
Mendez-Hernandez C. Use of glaucoma medications during pregnancy and breastfeeding. Arch Soc Esp Oftalmol 2012; 87: 389-391.
A general practitioner's approach
Dr Kate Kalloniatis BBioSc, MBBS, FRACGP, DCH
General Practitioner
Newcastle, NSW
Vascular work-up, papilloedema, hypertensive crisis and suspected thyroid eye disease.
Optometrists and general practitioners (GPs) play an important role in primary health care. This article aims to highlight a GP’s approach to preventative health activities around cardiovascular disease (CVD) and give a GP’s perspective on the management of hypertensive crisis, papilloedema and suspected thyroid eye disease (Graves’ ophthalmopathy).
Primary prevention is about identifying patients at risk prior to the development of disease. Vigilance on behalf of all clinicians involved in patient care can improve outcomes. CVD occurs in 18 per cent of Australians and accounts for 36 per cent of all deaths and 6.9 per cent of all disabilities.1
Our patients’ cardiovascular (CV) health can be determined by a number of modifiable and non-modifiable risk factors. Importantly, a number of modifiable risk factors associated with CVD also directly contributes to ocular complications like age-related macular degeneration (AMD), cataracts, inflammatory eye disease, thyroid eye disease, retinal ischemia, hypertensive retinopathy and diabetic eye disease.2–4
Which of your patients should be encouraged to see their GP?
A GP’s approach to evidence-based preventative health activities is outlined in The Royal Australian College of General Practitioners Guidelines for preventive activities in general practice 9th edition (Red Book).5 One of the primary screening tools utilised is the ‘assessment of absolute CVD risk’ which combines risk factors to calculate the probability that an individual will develop a cardiovascular event (myocardial infarction, stroke) or other vascular disease within five years.5
It is considered reasonable that we complete this assessment at least every two years in all adults aged over 45, or 35 for Aboriginal and Torres Strait Islander (ATSI) patients. Information required to complete this assessment includes the patient’s age, sex, smoking status, cholesterol (total and high-density lipoprotein-cholesterol), systolic blood pressure, diabetic status and the absence or presence of left ventricular hypertrophy (LVH). Using the Australian Cardiovascular disease charts (Figures 1 and 2) patients are stratified into Low (< 10 per cent), Moderate (10–15 per cent) and High Risk (> 15 per cent).
Evaluation of CVD risk generates discussion regarding modifiable risk factors and allows patients to focus on reducing these risk factors. This can be achieved through lifestyle changes, as well as appropriately prescribed pharmacotherapy like lipid-lowering agents, anti-hypertensives and medications directed towards smoking cessation.
In summary, all adults aged over 45—or 35 for ATSI patients—should be encouraged to see their GP for a CVD risk assessment and start the dialogue about how improving their modifiable risk factors can not only improve their ocular health but their general health as well.
Papilloedema
Papilloedema is defined as optic disc swelling that is due to raised intracranial pressure (ICP).6 It is an important examination finding which requires urgent investigation to determine the underlying cause.6 This sort of presentation requires careful evaluation by an appropriately-trained eye care professional to ensure that other causes of optic nerve swelling are excluded, and to differentiate true from pseudopapilloedema.7
The potential causes of raised ICP are varied and include intracranial mass lesions, cerebral oedema, increased cerebrospinal fluid (CSF) production, decreased CSF absorption, obstructive hydrocephalus, obstruction of venous outflow or idiopathic intracranial hypertension.6
To determine the cause of papilloedema the patient requires urgent neuroimaging and may also require a lumbar puncture, which is most efficiently arranged via the local Emergency Department. A GP could help facilitate this process, but given the urgency of the situation, they may not be immediately available. In some scenarios, it may be appropriate for the GP to arrange urgent outpatient imaging. Once the cause of the patient’s papilloedema has been determined, a GP’s strength is the co-ordination and oversight of appropriate longer-term follow-up.
Hypertensive crisis
From a preventative health point of view, a GP should aim to measure the blood pressure (BP) of any patient aged 18 years or older at least every two years. They interpret these BP measurements in the context of the patient’s absolute CVD risk assessment.5
In general, a GP is happy with BPs of ≤ 140/90 mmHg for adults and BP ≤ 130/80 mmHg for adults with a chronic disease.5 GPs generally act on high readings once a trend has been established: consistently high readings on two or more occasions.5 The exception is a patient presenting with a hypertensive crisis, which is a very uncommon presentation to a GP, but one not to be missed.
Most patients with significantly elevated blood pressure (systolic pressure ≥ 180 and/or diastolic pressure ≥ 120 mmHg) are well. This means they have no acute, end-organ injury (severe asymptomatic hypertension).8 Your clinical suspicion that a patient is in hypertensive crisis should be raised if you record a BP ≥ 180/ ≥ 120 mmHg and they are unwell. In broad terms, an unwell patient would exhibit concerning symptoms such as focal neurological symptoms (think: stroke), nausea/vomiting, any pain (headache, chest pain, abdominal pain, severe back pain), difficulty breathing and/or pregnancy (pre-eclampsia).8 Specific ocular examination findings would include evidence of moderate to severe hypertensive retinopathy (fresh flame haemorrhages, exudates [cotton-wool spots] or papilloedema).8
If the patient appears otherwise well with a high BP reading, it would be reasonable for them to review with their GP within 24-48 hours. If they are unwell, even if their BP is < 180/120 mmHg, it is likely they need urgent medical assessment. It is most appropriate to call an ambulance or ensure they can safely and quickly present to the local Emergency Department.
Graves’ disease is an autoimmune disorder involving the thyroid-stimulating hormone (TSH) receptor antibodies (TRAb). These antibodies essentially mimic the effects of TSH, thereby stimulating thyroid function, with the extrathyroidal TSH receptor expression linked with the pathogenesis of Graves’ ophthalmopathy.9,10
Graves’ ophthalmopathy is characterised by excessive tearing, periorbital oedema and proptosis. Extraocular muscle thickening and dysfunction can also lead to presentation of diplopia. Severe presentation can be sight-threatening related to optic nerve compression, elevated intra-ocular pressure due to elevated episcleral venous pressure or significant corneal ulceration primarily due to exposure. Graves’ ophthalmopathy affects approximately 20 per cent of those with a diagnosis of Graves’ disease. A patient’s presentation of Graves’ ophthalmopathy will often accompany clinical features of thyrotoxicosis.10
A GP would defer to an optometrist or an ophthalmologist to determine visual function, but management of vision-threatening Graves’ ophthalmopathy would require ophthalmological intervention. GPs are familiar with managing the non-ocular complications of Graves’ disease and assist in the diagnosis of Graves’ disease through initial investigations which include thyroid function tests, thyroid antibodies and if appropriate, a radionuclide thyroid scan.
GPs would commonly assess for clinical signs/symptoms of thyrotoxicosis which include tachycardia, hypertension, weight loss, diarrhoea, tremor, hyperreflexia, heat intolerance, anxiety and pretibial myxoedema.11 The symptom profile of a thyrotoxic patient can be quite broad with the severe end of the spectrum requiring urgent in-patient admission. For those patients who are amenable to outpatient treatment, GPs will often initiate treatment (carbimazole, beta blockers) and arrange outpatient specialist review to discuss definitive treatment such as radioactive iodine or surgery.9 Smoking leads to worsening of Graves’ ophthalmopathy10 and therefore smoking cessation is essential.
Ultimately, a GP wears two hats, and while there is much to be gained in preventative health, they are often at the forefront of the identification of acute medical illnesses which require urgent medical intervention. As colleagues and members of a multi-disciplinary care team, optometrists can also have an impact in identifying suitable cases for referral. By presenting a GP’s viewpoint, the hope is that a context for ongoing communication between clinicians will be provided and better patient care will be facilitated.
*Diabetes charts reproduced with permission from the National Heart Foundation of Australia from National Vascular Disease Prevention Alliance. Absolute cardiovascular disease risk management.
Quick reference guide for health professionals. Melbourne: NVDPA, 2012.
Visit the Australian absolute cardiovascular disease risk calculator (www.cvdcheck.org.au) for further education and information.
References
Australian Institute of Health and Welfare. Australia’s health 2006. Canberra: AIHW, 2006.
Solberg Y, Rosner M, Belkin M. The association between cigarette smoking and ocular diseases. Surv Ophthalmol 1998; 42: 535–547.
Fraser-Bell S, Symes R, Vaze A. Hypertensive eye disease: a review. Clin Exp Opthalmol 2017; 45: 45-53
Fraser C, D’Amico D, editors. Diabetic retinopathy: Prevention and treatment [internet]. Waltham, MA: UpToDate Inc.: 2018 [cited 2019 Feb 9]. Available from: https://www.uptodate.com/contents/diabetic-retinopathy-prevention-and-treatment
The Royal Australian College of General Practitioners. Guidelines for preventive activities in general practice. 9th edn, updated. East Melbourne, Vic: RACGP, 2018.
Bienfang D, editors. Overview and differential diagnosis of papilledema [internet]. Waltham, MA: UpToDate Inc.: 2019 [Cited 2019 Oct 3]. Available from: https://www.uptodate.com/contents/overview-and-differential-diagnosis-of-papilledema
Chiang J, Wong E, Whatham A et al. The usefulness of multimodal imaging for differentiating pseudopapilloedema and true swelling of the optic nerve head: a review and case series. Clin Exp Optom 2015; 98: 12-24
Elliott W, Varon J., editors.Evaluation and treatment of hypertensive emergencies in adults [internet]. Waltham, MA: UpToDate Inc.: 2019 [cited 2019 Sept 30]. Available from: https://www.uptodate.com/contents/clinical-features-and-diagnosis-of-graves-orbitopathy-ophthalmopathy
Ross D. Graves’ hyperthyroidism in nonpregnant adults: Overview of treatment. Post TW, ed. UpToDate. Waltham, MA: UpToDate Inc. https://www.uptodate.com (Accessed on October 03, 2019.)
Davies T, Burch H, editors. Clinical features and diagnosis of Graves’ orbitopathy (ophthalmopathy) [Internet]. Waltham, MA: UpToDate Inc.: 2019 [cited 2019 Oct 3]. Available from: https://www.uptodate.com/contents/clinical-features-and-diagnosis-of-graves-orbitopathy-ophthalmopathy
Ross D, editors. Overview of the clinical manifestations of hyperthyroidism in adults [Internet]. Waltham, MA: UpToDate Inc.: 2019 [cited 2019 Oct 3]. Available from: https://www.uptodate.com/contents/diagnosis-of-hyperthyroidism
Personalised medicines for eye care
Dr Alison Haywood BPharm PhD
School of Pharmacy and Pharmacology, Griffith University
Chris Testa BPharm BBus
Chris Testa’s Tugun Compounding Pharmacy
Beverley Glass BPharm BSc (Hons) PhD
Professor of Pharmacy, College of Medicine & Dentistry, James Cook University
Working with compounding pharmacists
Compounding, also referred to as ‘extemporaneous dispensing’ is the supply of a single ‘unit of issue’ of a therapeutic product intended for a specific person in response to an identified need.1,2
These compounded products are prepared in a community or hospital pharmacy and must be safe, efficacious and of a consistently high quality.1 The preparation of these compounded products is governed by a number of professional standards and guidelines1-4 and pharmacists are required to meet the Pharmacy Board of Australia and relevant state guidelines. No additional training or formal certification is required for a pharmacist to prepare compounded products.
Compounding pharmacists can work with optometrists and ophthalmologists to meet patient needs, when commercial products are not available or those commercially-available are not suitable for patients.2 Examples of requests for compounded preparations for eye care include antibiotics (gentamicin, tobramycin), antifungals (clotrimazole), antivirals (acyclovir) and N-acetylcysteine for cataracts.
How are eye drops compounded?
Ophthalmic products are sterile preparations that if prepared extemporaneously are governed by additional guidelines for ‘complex compounding’ since they involve special competencies, equipment, processes and facilities for their preparation.1,2,4 Criteria to provide quality, patient-centred compounding services are detailed in the Professional Practice Standards.2
The standard includes a compounding decision support and risk assessment tool (Figure 1) to assign a risk-rating related to the product, personnel and patient.2
Ingredients and formula
Ophthalmic products are sterile, liquid, semi-solid or solid preparations that may contain one or more active pharmaceutical ingredients (APIs) intended for application to the conjunctiva, the conjunctival sac or eyelids. A number of monographs for ophthalmic products exist in professional formularies such as the British Pharmacopoeia (BP), United States Pharmacopoeia (USP) and the Australian Pharmaceutical Formulary (APF).1 When a non-pharmacopoeial formula is used, the pharmacist is required to cite references relating to the stability, safety, and efficacy of the product.2 Since ophthalmic preparations are required to be sterile, an aseptic manufacturing process is usually employed, when the nature of the dosage form (for example: too viscous to filter) precludes the use of routine sterilisation methods.5
Sterilisation
Sterilisation is achieved by filtration (most applicable to use in a community pharmacy) or by heating in an autoclave, according to specifications detailed in the BP.1 Sterile compounding is required to be undertaken within cleanrooms and ancillary areas, using isolators, laminar flow cabinets, and laminar flow workbenches that meet Australian Standards, using protective clothing and equipment specifically designed for, and dedicated to, the preparation of these sterile products.4 Dedicated ingredients are required from approved sources (such as TGA-registered sources) and measuring equipment must be appropriately sterilised.2
Water for injections (sterile water used to dilute or dissolve drugs) is usually used as a vehicle for eye drops, and sodium chloride is added to ensure the drops are approximately isotonic with lachrymal secretion.1 Some formulas may require buffers, which need to be carefully selected, since they can reduce the stability of certain medicines if heat sterilisation is used.1 If a thickening agent is required, ingredients such as hypromellose 4500 may be added.1 Thickening agents moisten, soothe and lubricate the surface of eye and retain the drop on the eye for longer, however at high concentration their viscosity might make it difficult to sterilise the final product by filtration.6 Since patients can develop sensitivity to preservatives over time with repeated application of a product, alternative preservatives can be substituted or preservative-free single-use units may be used.1
Packaging
Compounders have access to a wide variety of packaging options that can be discussed with the prescriber to ensure stability of the product and to accommodate any patient preference. The volume of product in each container is generally limited to discourage prolonged storage.7
Tips for patients
The APF provides instructions for pharmacists on counselling patients on the appropriate administration of eye drops, ointments and gels; relevant cautionary advisory labels that are to be attached to the primary container.1 Flyers are also available online from Safe Medication.7 Pharmacists will also advise patients to store products away from children and pets. Ophthalmic products are generally required to be stored below 25°C, unless otherwise specified, for example where the API or other excipients in the product may be sensitive to elevated temperatures. The compounding pharmacist will also provide the patient with product information in the form of a Consumer Medicines Information (CMI) leaflet, which outlines safe use, storage and expiry.
Compounding atropine 0.01% eye drops
Control of myopia progression, particularly in children, has become an important goal, due to the increased global prevalence of myopia and the increased risk for ocular pathology associated with high myopia.8,9 A recent review of the epidemiology and pathophysiology in myopia by Wu et al8 highlights clinical trials using atropine in school-aged children. Recent clinical trials have demonstrated that low-dose atropine (0.01%) slows myopia progression, with significantly less side-effects compared to higher concentration preparations.8,10
Note: Low-dose atropine (0.01%) eye drops are not commercially available, and may be prepared by a compounding pharmacist in appropriate sterile facilities.
When a prescriber requests atropine 0.01% eye drops
The following case outlines the process that a compounding pharmacist would take when presented with a request from the prescriber. (Figure 2 provides an example prescription). It is important that the prescriber clearly states on the prescription that the product is to be compounded, to prevent the accidental dispensing of the commercial 1% product. The existing commercial product (Atropt Eye Drops) cannot be used since it contains 100 times the concentration of atropine (Table 1).
Can the commercial product be diluted?
While the commercial product could be diluted to contain the correct amount of atropine, and sterility can be maintained via filtration, dilution will have altered the concentration of excipients present with potential to affect both the stability and solubility of the atropine and the preservative efficacy as well as the consistency (thickness).
Step 1. Design of an appropriate formula
A drug (salt) is chosen based on its solubility and stability: Atropine sulfate a weakly basic drug, which has the following solubilities in 100 mL (water 0.22g; ethanol 50g; glycerol 3.70g).11 Degradation of atropine sulfate is primarily due to hydrolysis, with the rate of hydrolysis increasing at temperatures above that of room temperature. Stability and solubility is thus optimum for aqueous atropine in an acid solution (pH 3-4).12 Atropine sulfate is also susceptible to light degradation and this should be reflected on in the choice of the immediate container and/or advice to protect the product from light during preparation and during use by the patient.6
Step 2. The form of the drug that will be used to compound the product is chosen
Pure raw material may be used, but this is limited by the amount that can be weighed accurately (due to capacity of the balance). A commercial product for example, a 0.6 mg/ml and 1.2 mg/ml injection, which may also be used as a source of atropine, has the added advantage that it is sterile.
Step 3. The excipients to deliver and optimise the stability of the drug are chosen.
These are included to preserve the solution (benzalkonium chloride, disodium edetate, benzyl alcohol) maintain pH at about 4.5 (boric acid, sulphuric acid, hydrochloric acid) and maintain isotonicity (sodium chloride).
Best practice standards are applicable to all pharmacists, no matter the level of complexity of the compounding undertaken. Figure 3 details processes that pharmacists undertake for complex compounding from an internal or external audit for assessing risk in terms the pharmacy, product, staff and patients.
Optometrists interested in prescribing compounded products should identify a pharmacy equipped to compound sterile preparations, since these products require specialised equipment and facilities. (The current PBS List on the Optometry Australia website, provides a brief state-by-state directory of ophthalmic compounding pharmacists). A visit to the compounding pharmacy will provide the prescriber with further confidence that the pharmacy will be able to provide a service to meet the eye care needs of their patients.
References
Sansom L. N. ed. Australian pharmaceutical formulary and handbook, 24th ed. Canberra: Pharmaceutical Society of Australia; 2018.
Pharmaceutical Society of Australia. Professional Practice Standards, Version 5, 2017. Available from: https://www.psa.org.au/wp-content/uploads/2018/08/Professional-Practice-Standards-v5.pdf.
Pharmaceutical Society of Australia. National competency standards framework for pharmacists in Australia, 2016. Available from: https://www.psa.org.au/wp-content/uploads/2018/06/National-Competency-Standards-Framework-for-Pharmacists-in-Australia-2016-PDF-2mb.pdf.
Pharmacy Board of Australia. Codes, Guidelines and Policies. Available from: https://www.pharmacyboard.gov.au/Codes-Guidelines.aspx.
World Health Organization. Ophthalmic products. The International Pharmacopoeia, 8th ed, 2018. Available from: http://apps.who.int/phint/en/p/docf/.
Martindale: The complete drug reference (electronic resource). London: Pharmaceutical Press; 2019.
American Society of Health-System Pharmacists. Safe Medication. Available from: http://www.safemedication.com/safemed/docs/Eye-Drop-Flyer.pdf.
Wu PC, Chuang MN, Choi J, et al. Update in myopia and treatment strategy of atropine use in myopia control. Eye (Lond) 2019; 33(1): 3-13.
Parry N. How to use low-dose atropine to slow myopic progression in kids. EyeNet Magazine 2016: 29-31.
Chia A, Lu QS, Tan D. Five-year clinical trial on atropine for the treatment of myopia 2: Myopia control with atropine 0.01% eyedrops. Ophthalmology 2016; 123(2): 391-399.
National Institutes of Health PubChem. Atropine sulfate. Solubility. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Atropine-sulfate#section=Solubility.
Schier JG, Ravikumar PR, Nelson LS, et al. Preparing for chemical terrorism: stability of injectable atropine sulfate. Acad Emerg Med 2004; 11(4): 329-334.
Australian Register of Therapeutic Goods. Minims Atropine EyeDrops Consumer Medicine Information. Available from: https://www.ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2018-CMI-01359-1.
Australian Register of Therapeutic Goods. Atropt Consumer Medicine Information. Available from: https://www.ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2010-CMI-01572-3&d=201907231016933.
December 2019
Contact lens prescribing trends 2019
Professor Emeritus Nathan Efron AC DSc PhD BScOptom FAAO(Dip CCLRT) FCCLSA FACO
Professor Emeritus, Institute of Health and Biomedical Innovation, and School of Optometry, QUT, Brisbane, Australia
Professor Philip B Morgan PhD Eurolens Research, the University of Manchester, Manchester, UK
Professor Craig A Woods PhD School of Medicine (Optometry), Deakin University, Geelong, Australia
The 20th annual survey of Australian contact lens prescribing was conducted during the first three months of 2019.
The same format as in previous years was employed. An email was sent to all members of Optometry Australia with a link to a questionnaire, and a request that this be downloaded, printed and completed to provide details of the first ten patients fitted with contact lenses after receipt of the questionnaire. The survey was specifically designed to be straightforward to complete while capturing key patient information.
Practitioners were asked general questions about themselves. For each contact lens fitting, they were requested to complete the following details: date of fitting, new fitting or refitting, age and sex of patient, lens material, lens design, frequency of replacement, times per week of wear, modality (daily or extended wear) and care system. Practitioners were asked to return the photographed or scanned copies of the questionnaire by email.
Completed questionnaires relating to 502 contact lens fits were returned, which provides a sound basis for a meaningful analysis. Each fitting was given an annualised weighting based on the number of lenses fitted during the survey period and the time taken to complete the fits. This means that data generated by practitioners with a higher frequency of fitting contact lenses were afforded a higher weighting than those with a lower frequency of fits.
The discussion below will concentrate primarily on data relating to new lens fits, as opposed to refits. We believe that new fits are a more sensitive barometer of current patterns and future trends, whereas refits are more indicative of previous fitting behaviours.
In keeping with other markets around the world,1 a majority of lenses (65 per cent) were fitted to females. The average age of contact lens wearers at the time of fitting has increased over the past two decades, from 32 in 2000 to 37.0 ± 17.4 years this year. The age at fitting ranged from 1 to 89 years.
Soft lens materials and designs
Soft lenses are still the main type of contact lens fitted, accounting for 90 per cent of new fits; soft lenses have represented the vast majority of contact lens fits since our survey began two decades ago.2
Figure 1 is a composite of pie charts detailing the key findings of the 2019 survey in relation to soft lenses. Silicone hydrogels are still the dominant material, representing 79 and 80 per cent of materials prescribed as new fits and refits, respectively, with the balance comprising mainly of mid- and high-water content hydrogel materials.
Figure 1. Detailed results for soft contact lens prescribing in the 2019 Australian survey (Si-H: silicone hydrogel; WC: water content).
The key categories of lens designs are spherical, toric, multifocal, monovision, coloured (tinted) and myopia control. Spherical and toric designs each represented 26 per cent of new fits (Figure 1).
Figure 2 shows trends in contact lens materials prescribed over the past two decades. It can be seen that there was a gradual increase in silicone hydrogel prescribing from 2000 to 2017, which has remained steady since then. The reason for the popularity of this highly oxygen-permeable material type is that it essentially eliminates hypoxic complications such as limbal and conjunctival redness, stromal oedema, corneal neovascularisation and epithelial microcysts.3
Figure 2. Proportion of all fits of various soft lens material types in Australia between 2000 and 2019 (Si-H: silicone hydrogel; WC: water content)
Multifocal designs (27 per cent of new fits) continue to be preferred to monovision (four per cent) for the correction of presbyopia. This trend, which has been evident since the turn of the century, largely can be attributed to improved multifocal lens designs. The fact that almost one-third of soft lens fits are for the correction of presbyopia highlights the importance of this growing demographic in modern day contact lens practice.
Coloured (tinted) lenses do not seem to be popular in Australia; in fact, no coloured lens fits were recorded in our 2019 survey.
Myopia control lenses incorporate special designs for arresting the rate of progression of myopia.4 This year saw a sudden surge of interest in prescribing for myopia control, with such lenses representing 17 per cent of new fits. This sudden increase may be related to the recent introduction into Australia of the MiSight lens (CooperVision), which is specifically designed for myopia control. As well, the considerable discussion and debate in the literature, at conferences and in online forums has undoubtedly fuelled interest in this modality of lens correction.
Soft lens replacement and wearing modality
Virtually all soft lenses are replaced daily (63 per cent) or monthly (28 per cent). Trends since 2000 in soft lens fitting according to replacement frequency are shown in Figure 3. Daily disposable lenses now dominate the Australian market, with the level of prescribing of this modality remaining relatively constant at above 60 per cent since 2015.
Figure 3. Proportion of all fits of soft lens lenses according to replacement frequency in Australia between 2000 and 2019
Extended wear lens fitting, almost exclusively with silicone hydrogel materials, has remained constant at under 10 per cent of all lens fits over the past decade, and has dropped to a low point of five per cent of all lens fits in 2019.
Multi-purpose solutions are now used almost exclusively by those wearing reusable lenses, with this solution type representing 98 per cent of prescribed care regimens. The balance is peroxide systems.
Australia versus the world
We conduct annual contact lens fitting surveys in about 40 countries each year.1 This provides an opportunity to benchmark against international colleagues, and this year we compare contact lens prescribing in Australian against world trends (the latter derived from 2018 data1) (Figure 4). Seven key categories of lens type are represented. The outer and inner rings display the Australian and world-wide fitting data,1 respectively.
Perhaps the greatest difference revealed in Figure 4 is that daily disposable silicone hydrogel lenses – widely believed to be the most advanced lens type in terms of eye health – are prescribed at more than twice the rate in Australia (35 per cent) compared with the rest of the world (17 per cent). Australia has always been recognised as being at the forefront of contact lens prescribing, with Australian optometrists being ‘early adopters’ of new technologies. As well, the rate of rigid lens prescribing is higher in Australia than world averages.
Figure 4. Percentage of all contact lenses prescribed in Australia (2019, outer ring) compared with the world (2018, inner ring). (EW: extended wear; Si-H: silicone hydrogel; DD: daily disposable; OK: orthokeratology).
Conclusions
The results of our 2019 survey confirm the ongoing high rate of prescribing of silicone hydrogel materials and daily disposable lenses in Australia. The sudden spike in prescribing of lenses for myopia control is perhaps the stand-out highlight of our 20th anniversary report; it will be interesting to see if this very high rate of prescribing of this lens type is sustained into the future.
References
Morgan PB, Woods CA, Tranoudis IG et al. International contact lens prescribing in 2018. Contact Lens Spectrum 2019; 34: 26-32.
Morgan PB, Efron N, Helland M et al. How does the UK market compare with other countries? Optician 2001; 221: 26-32.
Efron N. Contact Lens Complications. 4th edition. Edinburgh: Elsevier, 2019.
Sankaridurg P. Contact lenses to slow progression of myopia. Clin Exp Optom 2017; 100: 432-437.
Contact lenses: beyond 20/20
Dr Lyndon Jones PhD DSc FCOptom FAAO
Deborah Jones BSc FCOptom FAAO
Centre for Ocular Research and Education (CORE), School of Optometry & Vision Science, University of Waterloo, Ontario, Canada
Rebecca Jones BSc
Michael G. DeGroote
School of Medicine, McMaster University, Cairns Family Health and Bioscience Research Complex, Ontario, Canada
A look forward to the emerging innovations in contact lenses — from the control of myopia progression to the detection and treatment of ocular disease. It’s all closer than you’d think.
The use of contact lenses continues to grow, with an estimated 140 million wearers globally. While the majority of wearers use contact lenses for the correction of refractive error, there is growing interest in their use for ‘non-standard’ concepts. As we approach the magical year (for optics) of 2020, we ask: if we glimpse into the future, what will the contact lenses of (say) 2035 look like? What options will they provide to our patients that will differ from the lenses of today?1
Myopia control
Myopia is a significant public health problem. In 2010 it was estimated that 28 per cent of the world’s population was myopic, but it is predicted that by 2050, 50 per cent of the global population could be myopic.2 As discussed in the September issue of Pharma, the most rapid increase has been in East Asian countries, where it has already reached epidemic proportions, affecting over 90 per cent of adults in some regions such as Korea, Taiwan and Singapore.3 Myopia is not merely an inconvenience resulting in the patient requiring an optical correction. The myopic eye, particularly those with high myopia of > 6.00 D, has an increased risk of developing ocular pathology that may lead to vision loss, in particular retinal detachment and myopic macular degeneration. Thus, methods to slow or prevent myopia progression (and the ocular axial elongation that accompanies it) are extremely important if myopia-induced pathologies are to be avoided. Recent estimates suggest that slowing myopia progression by one dioptre should reduce the likelihood of a patient developing myopic maculopathy by 40 per cent.4
Several treatment paradigms for slowing myopia progression have been evaluated in intervention studies, largely encompassing the use of either pharmacological means (most commonly through the use of the topical anti-muscarinic drug atropine) or various optical interventions.5-13 These optical interventions include progressive addition spectacle lenses, bifocal spectacles, orthokeratology rigid contact lenses and multifocal soft contact lenses.8,14-19
To date, many of the contact lens methods used remain ‘off-label,’ meaning that while studies would suggest that such technologies do indeed appear to show a slowing of myopia progression, regulatory approvals for these products do not yet exist to support the product being used in such a manner.20 One such example is orthokeratology, which is approved for use in the reduction of refractive error, but not approved for slowing the progression of myopia, despite many studies supporting this to be the case.
However, as the interest in using contact lenses for slowing myopia progression increases, more products will gain regulatory approval for this indication, resulting in this being a significant growth area for contact lenses over the next decade. Two commercially available daily disposable soft lens products that have gained regulatory approval for slowing the progression of myopia in various countries following successful clinical trials are MiSight (CooperVision)21 and NaturalVue Multifocal (Visioneering Technologies).22
Drug delivery
One of the biggest opportunities for the development of ‘specialised’ contact lenses relates to their use as drug delivery devices. A lens that would release therapeutically-relevant doses of a topical drug for five-to-seven days would likely find an immediate place in clinical practice and there is great interest in this concept among clinicians.23 The interest in this topic is evidenced by the fact that over 350 peer-reviewed publications have addressed this issue, with 25 per cent of them being published within the last five years. This is particularly relevant for diseases which require consistent dosing over many weeks or months, in which compliance with instilling drops becomes lower over time, for example in the management of glaucoma.24
Several research groups around the globe are actively looking at developing such technologies. There are various methods proposed to deliver ocular medications, with many employing novel approaches based on nanotechnology.25 Recent publications on this topic include those describing the extended release of anti-glaucoma medications,26 antibiotics,27-29 antifungal agents,30,31 drugs to treat dry eye and surface inflammation,32 drugs to slow the progression of myopia33 and anti-inflammatory drugs.34,35 Contact lenses have already been used in full-scale clinical trials that release an anti-allergic agent (ketotifen).36
Based upon the rapidly expanding literature in this field and the level of interest, it appears to be just a matter of time before such devices become commercially available. However, concerns relating to regulatory approvals, how to control the leaching of drugs into the surrounding blister pack solution and which practitioners are licensed to dispense such products will likely delay their introduction for some time while these issues are addressed.
Detection and monitoring of disease
The ability of contact lenses to monitor ocular and systemic diseases such as diabetes and glaucoma would appear to be something approaching science fiction. However, there is growing interest in the use of wearable sensors for many aspects of health monitoring.37-39 There is already a commercially-available contact lens device (Figure 1) that uses sophisticated strain-gauge technology to continuously measure intraocular pressure over a 24-hour time period,40,41 and several groups have published work on the development of materials that can monitor glucose levels within the tear film.42-44 Published work has also looked at using the tear film to monitor signs of cancer45,46 and contact lenses that could detect such small levels of biomarkers within the tear film would be invaluable.47 Thus, the continued expansion of interest in the development of such devices seems inevitable, as developments in miniaturisation of batteries and electrical components improves.48,49
Advanced optical designs
The final area of interest relates to the manufacture of lenses with novel optics. Spectacle-mounted head-up displays with the ability to access the internet, display websites and email, stream video or take photographs have been under development for several years, with the most well-known being the Google Glass concept, launched in 2013.
Other manufacturers have worked on various versions of these ‘smart spectacle’ platforms and the development of newer technologies have enabled companies to consider incorporating this technology into a contact lens platform. This concept could be used to develop, for example, a multifocal contact lens that changes power depending upon the distance at which the wearer is viewing an item of interest, a magnifying contact lens for people with low vision and even opens up the potential for almost invisible virtual reality systems that offer great improvements over the current bulky, head-mounted versions.50-54
The future for contact lenses remains bright, with many new and exciting developments ahead. Contact lenses to control myopia progression are already here and the number of options will rapidly expand; in the near future, lenses to detect and treat ocular disease will be available and in the more distant future, we are likely to see the availability of lenses with highly sophisticated optics for unique optical applications.
Disclosure
This manuscript was not specifically funded by any grant or contract. Over the past year, CORE has received research grants from Alcon, Allergan, CooperVision, GLChemtech, Johnson & Johnson Vision, Menicon, Novartis, PS Therapy, Shire and Sightglass outside the submitted work. Lyndon Jones has received personal fees from Alcon, CooperVision, Johnson & Johnson Vision, Menicon, Novartis and Ophtecs outside the submitted work. Deborah Jones has received personal fees from CooperVision. The authors report no other conflicts of interest in this work.
References
Jones LW, Chauhan A et al. Expert Views on Innovative Future Uses for Contact Lenses.Optom Vis Sci 2016; 93: 328-335.
Holden BA, Fricke TR et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050.Ophthalmology 2016; 123: 1036-1042.
Pan CW, Dirani M et al. The age-specific prevalence of myopia in Asia: a meta-analysis.Optom Vis Sci 2015; 92: 258-66.
Bullimore MA, Brennan NA. Myopia Control: Why Each Diopter Matters.Optom Vis Sci 2019; 96: 463-465.
Gong Q, Janowski M et al. Efficacy and Adverse Effects of Atropine in Childhood Myopia: A Meta-analysis.JAMA Ophthalmol 2017; 135: 624-630.
Pineles SL, Kraker RT et al. Atropine for the Prevention of Myopia Progression in Children: A Report by the American Academy of Ophthalmology.Ophthalmology 2017; 124: 1857-1866.
Huang J, Wen D et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis.Ophthalmology 2016; 123: 697-708.
Wildsoet CF, Chia A et al. IMI – Interventions Myopia Institute: Interventions for Controlling Myopia Onset and Progression Report.Invest Ophthalmol Vis Sci 2019; 60: M106-M131.
Sankaridurg P, Conrad F et al. Controlling Progression of Myopia: Optical and Pharmaceutical Strategies.Asia Pac J Ophthalmol (Phila) 2018; 7: 405-414.
Tran HDM, Tran YH et al. A Review of Myopia Control with Atropine.J Ocul Pharmacol Ther 2018; 34: 374-379.
Cho P, Tan Q. Myopia and orthokeratology for myopia control.Clin Exp Optom 2019; 102: 364-377.
Prousali E, Haidich AB et al: Efficacy and safety of interventions to control myopia progression in children: an overview of systematic reviews and meta-analyses.BMC Ophthalmol 2019; 19: 106.
Weiss RS, Park S. Recent updates on myopia control: preventing progression 1 diopter at a time.Curr Opin Ophthalmol 2019; 30: 215-219.
Gifford P, Gifford KL. The Future of Myopia Control Contact Lenses.Optom Vis Sci 2016; 93: 336-343.
Turnbull PR, Munro OJ et al. Contact Lens Methods for Clinical Myopia Control.Optom Vis Sci 2016; 93: 1120-1126.
Xie P, Guo X. Chinese Experiences on Orthokeratology.Eye Contact Lens 2016; 42: 43-7.
Leo SW, Scientific Bureau of World Society of Paediatric O, et al.: Current approaches to myopia control.Curr Opin Ophthalmol 2017; 28: 267-275.
Sankaridurg P. Contact lenses to slow progression of myopia.Clin Exp Optom 2017; 100: 432-437.
Jones L, Drobe B et al. IMI – Industry Guidelines and Ethical Considerations for Myopia Control Report.Invest Ophthalmol Vis Sci 2019; 60: M161-M183.
Chamberlain P, Peixoto-de-Matos S et al. A 3-Year Randomized Clinical Trial of MiSight Lenses for Myopia Control.Optom Vis Sci 2019; In press.
Cooper J, O’Connor B et al. Case Series Analysis of Myopic Progression Control With a Unique Extended Depth of Focus Multifocal Contact Lens.Eye Contact Lens 2018; 44: e16-e24.
Karlgard CC, Jones LW et al. Survey of bandage lens use in North America, October-December 2002.Eye Contact Lens 2004; 30;1: 25-30.
Davis SA, Sleath B et al. Drop instillation and glaucoma.Curr Opin Ophthalmol 2018; 29: 171-177.
Hui A, Willcox M. In Vivo Studies Evaluating the Use of Contact Lenses for Drug Delivery.Optom Vis Sci 2016; 93: 367-376.
Xu J, Ge Y et al. Co-delivery of latanoprost and timolol from micelles-laden contact lenses for the treatment of glaucoma.J Control Release 2019; 305 18-28.
Maulvi FA, Singhania SS et al. Contact lenses with dual drug delivery for the treatment of bacterial conjunctivitis.Int J Pharm 2018; 548: 139-150.
Postic I, Sheardown H. Altering the release of tobramycin by incorporating poly(ethylene glycol) into model silicone hydrogel contact lens materials.J Biomater Sci Polym Ed 2019; 30: 1115-1141.
Phan CM, Bajgrowicz-Cieslak M et al. Release of Moxifloxacin from Contact Lenses Using an In Vitro Eye Model: Impact of Artificial Tear Fluid Composition and Mechanical Rubbing.Transl Vis Sci Technol 2016; 5: 3.
Gallagher AG, McLean K et al. Development of a Poly-epsilon-Lysine Contact Lens as a Drug Delivery Device for the Treatment of Fungal Keratitis.Invest Ophthalmol Vis Sci 2017; 58: 4499-4505.
Phan CM, Bajgrowicz M et al. Effects of Antifungal Soaked Silicone Hydrogel Contact Lenses on Candida albicans in an Agar Eye Model.Eye Contact Lens 2016; 42: 313-317.
Choi JH, Li Y et al. The Efficiency of Cyclosporine A-Eluting Contact Lenses for the Treatment of Dry Eye.Curr Eye Res 2019; 44: 486-496.
Hui A, Bajgrowicz-Cieslak M et al. In vitro release of two anti-muscarinic drugs from soft contact lenses.Clin Ophthalmol 2017; 11 1657-1665.
Rad MS, Sajadi Tabassi SA et al. Controlled release of betamethasone from vitamin E-loaded silicone-based soft contact lenses.Pharm Dev Technol 2016; 21: 894-899.
Torres-Luna C, Hu N et al. Extended delivery of non-steroidal anti-inflammatory drugs through contact lenses loaded with Vitamin E and cationic surfactants.Cont Lens Anterior Eye 2019.
Pall B, Gomes P et al. Management of Ocular Allergy Itch With an Antihistamine-Releasing Contact Lens.Cornea 2019; 38: 713-717.
Alharbi M, Straiton N et al. Data management and wearables in older adults: A systematic review.Maturitas 2019; 124: 100-110.
Huang H, Su S et al: Graphene-Based Sensors for Human Health Monitoring.Front Chem 2019; 7: 399.
Cho J. Current Status and Prospects of Health-Related Sensing Technology in Wearable Devices.J Healthc Eng 2019; 2019: 3924508.
Mansouri K, Medeiros FA et al. Continuous 24-hour monitoring of intraocular pressure patterns with a contact lens sensor: safety, tolerability, and reproducibility in patients with glaucoma.Arch Ophthalmol 2012; 130: 1534-9.
Marando CM, Mansouri K et al. Tolerability and Functionality of a Wireless 24-Hour Ocular Telemetry Sensor in African American Glaucoma Patients.J Glaucoma 2019; 28: 119-124.
Ascaso FJ, Huerva V. Noninvasive Continuous Monitoring of Tear Glucose Using Glucose-Sensing Contact Lenses.Optom Vis Sci 2016; 93: 426-434.
Park J, Kim J et al. Soft, smart contact lenses with integrations of wireless circuits, glucose sensors, and displays.Sci Adv 2018; 4: eaap9841.
Lin YR, Hung CC et al. Noninvasive Glucose Monitoring with a Contact Lens and Smartphone.Sensors (Basel) 2018; 18: 10.
Evans V, Vockler C et al. Lacryglobin in human tears, a potential marker for cancer.Clin Experiment Ophthalmol 2001; 29: 161-163.
de Freitas Campos C, Cole N et al. Proteomic analysis of dog tears for potential cancer markers.Res Vet Sci 2008; 85: 349-352.
Hagan S, Martin E et al: Tear fluid biomarkers in ocular and systemic disease: potential use for predictive, preventive and personalised medicine.EPMA J 2016; 7: 15.
Phan CM, Subbaraman L et al. The Use of Contact Lenses as Biosensors.Optom Vis Sci 2016; 93: 419-425.
Kobashi H, Ciolino JB. Innovative Development of Contact Lenses.Cornea 2018; 37 Suppl 1 S94-S98.
Milton HE, Morgan PB et al. Electronic liquid crystal contact lenses for the correction of presbyopia.Opt Express 2014; 22: 8035-8040.
Schuster GM, Arianpour A et al. Wink-controlled polarization-switched telescopic contact lenses.Appl Opt 2015; 54: 9597-9605.
Kaur S, Kim YJ et al. Graphene electrodes for adaptive liquid crystal contact lenses.Opt Express 2016; 24: 8782-8787.
Wu Y, Chen CP et al. Design of retinal-projection-based near-eye display with contact lens.Opt Express 2018; 26: 11553-11567.
Bailey J, Morgan PB et al. Switchable Liquid Crystal Contact Lenses for the Correction of Presbyopia.Crystals 2018; 8: 29.
Red eye conditions
Red eye reference guide
Reprinted from the 2019 Optometry Australia anterior eye Clinical Practice Guide for the diagnosis, treatment and management of anterior eye conditions, this reference guide covers the diagnosis and management of bacterial keratitis, herpes simplex keratitis and acute anterior uveitis.
Visiting Research Fellow, Queensland University of Technology
The IMI has a message for eye-care professionals: it’s no longer best practice to simply prescribe single vision spectacles for progressing myopes.
The International Myopia Institute (IMI) White Paper Reports were published in the high-ranking journal Investigative Ophthalmology and Visual Science in February 2019. In a similar spirit to the Tear Film and Ocular Surface Society Dry Eye Workshop (TFOS DEWS and DEWS II) reports, the IMI Reports present a comprehensive peer consensus from over 85 participant authors on a wide scope of topics relating to research of myopia mechanisms, product research and development, clinical and industry best practice and the public health message. The IMI Reports are open-access and freely available, creating a clear picture of the current landscape of myopia research and practice, with an eye to the future.
The IMI Reports have come at exactly the right time. Over the past few years there has been a dramatic increase in clinician awareness and product innovations by industry to match the research findings of a global increase in the prevalence of myopia, forecast to affect 50 per cent of the world’s population by 2050.¹ The well-informed optometrist would benefit from reading any and all of the IMI Reports, however, if pressed for time, the place to start is the Myopia Control Reports Overview and Introduction, which details the background of risk factors for myopia onset and progression, along with providing an overview of each report to direct further learning. From there, essential practitioner reading includes the following Reports:
Defining and Classifying Myopia – Get clear on the definitions of pre-myopia, myopia, high myopia, and myopia complication with key references.²
Interventions for Myopia Onset and Progression – Understand the research behind optical, pharmacological, environmental (behavioural) and surgical interventions for myopia.³
Clinical Management Guidelines – Appreciate the scope of risk identification, parent and patient communication, informed consent, basic examination procedures, follow-up schedules, when to change and stop treatment, future treatments and additional resources for clinical practice.⁴
Industry Guidelines and Ethical Considerations for Myopia Control – Consider factors in the ethical development, registration, marketing, on- and off-label prescribing and patient use of myopia control treatments, including risk versus benefit and quality of life considerations.⁵
The Clinical Management Guidelines (CMG) Report⁴ provides a framework for putting research into practice. Best practice myopia management involves an understanding of the causes and risk factors for myopia; the long-term eye health risks; the efficacy and safety of the available optical, pharmacological and visual environment interventions; and the skills to translate this into lay language for both the patient and parent. The CMG Report commences with an outline of myopia development causes—identifying the pre-myope—through the risk factors of family history (one or two myopic parents), less time spent outdoors and specific binocular vision disorders (esophoria and accommodative lag). The key identifier of the pre-myope, though, is the child who is less hyperopic than age normal; specifically: a child who is +0.75 or less at age 6–7 years.
Evidence-based interventions for this child are currently limited to education on achieving around 90+ minutes of time outdoors per day. Managing binocular vision disorders associated with myopia onset may also be beneficial, although specific studies on delaying myopia with this sort of intervention have not been undertaken.
Management
Once a child becomes myopic, a management strategy should be instigated which not just corrects myopia but also aims to slow its progression. Based on the available evidence, this can be implemented for children as young as six years of age and should continue until the mid-to-late teens, although rebound effects on treatment cessation and young adult myopia progression are both yet to be fully understood.
Figure 1. Clinical tests in myopia management, published from the IMI Clinical Management Guidelines
The CMG Report provides guidance firstly on discussing myopia and its treatments—options, efficacy, safety, additional corrections and informed consent—while emphasising the importance of establishing reasonable expectations and informed consent (Chapters two and three). The report then proceeds to the key elements of the baseline exam for myopia control (Chapter four; see Figure 1 of the CMG Report, and Figure 2). The standard procedure for examination includes appropriate history taking relative to the treatment, distance and near acuity, subjective and/or objective refraction, accommodative and binocular vision assessment and ocular health examination. Cycloplegic refraction is considered useful annually, or as indicated. Fundus examination through dilated pupils is also suggested as an annual exam component, especially for high myopes (> 5 D) and/or if axial length is 26 mm or greater.
Figure 2. Clinical review schedules based on treatment type, adapted from the IMI Clinical Management Guidelines.
While axial length measurement is considered a necessity for a research study, for clinical practice it is currently considered preferable, but not a necessity, every six months. This is a particular issue with orthokeratology (OK) treatment where refractive change is more difficult to measure; and with atropine therapy where a mismatch between axial length and refractive control has been repeatedly noted. These two treatments also carry their own specific recommendations for follow-up examination—OK monitoring requires corneal topography, and atropine monitoring requires assessment of pupil size and function and intraocular pressure.
The bulk of the CMG Report is then dedicated to selecting a treatment strategy and management guidelines. Considering a child’s baseline refractive error (for example, astigmatism limits certain contact lens treatments) and capacity is important alongside treatment consideration such as advice on add powers in multifocal soft contact lenses and detail on spectacle lens options (Chapter 5).
Guidelines for clinical care (Chapter 6) detail all aspects of treatment and advice from ideal wearing time (at least five to six days a week, dependent on the treatment), back up corrections, advice on visual environment, when to change or end treatment and special considerations such as late onset and high myopia. A summary of follow-up schedules by treatment is provided in Figure 2. The CMG Report concludes with information on clinical references – key research papers, websites, courses and communication tools – where much is provided as weblinks in the supplementary digital content.
Looking to the future
The report holds more promise for the influence that current research may have on future clinical practice. The myopia managing clinician of the future may be measuring parameters such as relative peripheral refraction, aberrometry, pupillometry, sub-foveal choroidal thickness and utilising light exposure and visual activity data from wearable devices (Chapter 4). Each of these is an arena for current research and as their role in predicting myopia progression or treatment response is understood, these may translate into clinical practice. The hot topics of OK and multifocal soft contact lens optimisation are detailed in Chapter 7, along with emerging treatments such as the 7-methylxanthine nutritional supplement in Denmark and scleral reinforcement in Russia.
Conclusion
The publication of the IMI White Paper Reports is a landmark moment for the eye-care profession and industry. By providing a full-scope, critically-evaluated and robustly synthesised expedition through the world of myopia research and practice, these reports clearly draw a line in the sand for future coordinated efforts for the ultimate benefit of our young myopic patients.
The clear message for eye-care professionals right across the world is that it’s no longer best practice to simply prescribe single vision spectacles for progressing myopes when better options to control myopia are available. Myopia management, at minimum, starts with a discussion on the consequences of myopia, risk factors and treatments—allowing parents and patients to make informed decisions which could influence lifelong eye health outcomes. While there is no way to predict the level of progression or perfect treatment for the individual myope—and there may never be—there are many tools and treatments available.
Improving the access of our young myopic patients and their parents to the right information and treatments is built on a foundation of practitioner education and confidence in implementation. The IMI White Papers, and particularly the Clinical Management Guidelines, are designed to support practitioners through this imperative evolution of clinical practice.
Dr Gifford (PhD BAppSc (Optom) Hons GCOT FBCLA FIACLE FCCLSA FAAO) is a clinician-scientist in Brisbane private practice, a peer educator, and a Visiting Research Fellow at the Queensland University of Technology. She is the Chair of the Clinical Management Guidelines Committee of the International Myopia Institute and lead author on their report.
References
1. Holden BA, Fricke TR, Wilson DA et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016; 123: 1036-1042
2. Flitcroft DI, He M, Jonas JB et al. IMI – Defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019; 60: M20-M30.
3. Wildsoet CF, Chia A, Cho P et al. IMI – Interventions for Controlling Myopia Onset and Progression Report. Invest Ophthalmol Vis Sci. 2019; 60: M106-M131.
4. Gifford KL, Richdale K, Kang P et al. IMI – Clinical Management Guidelines Report. Invest Ophthalmol Vis Sci. 2019; 60: M184-M203.
5. Jones L, Drobe B, González-Méijome JM et al. IMI – Industry Guidelines and Ethical Considerations for Myopia Control Report. Invest Ophthalmol Vis Sci. 2019; 60: M161–M183.
Key resources with links
Blog
To read more on axial length in clinical practice, the author has written a blog entitled ‘Axial length measurement – a clinical necessity?’
The International Myopia Institute – a summary of prevalence, impact and solutions for the global myopia problem, with information on the Committees and links to the White Paper Reports. (myopiainstitute.org )
The website Myopia includes easy access to the CMG Supplementary Digital Content and a new podcast series with IMI Report lead authors, along with numerous educational blogs and resources for putting myopia management into practice (myopiaprofile.com)
The BHVI Global Myopia Centre, a portal to online courses, calculators and resources.
Issue 47 of ContactLensUpdate.com, entitled ‘Myopia Matters: Summarising the IMI Reports’. This free-to-access resource includes an editorial written by this author, a summary of each of the white papers by the researchers of the Centre for Ocular Research and Education (CORE – University of Waterloo, Canada) and a practitioner reference factsheet download on the Clinical Management Guidelines.
The companion Facebook Group ‘Myopia Profile’, administered by the author – a closed, industry-only group which includes more than 5,000 eye care practitioners from over 50 countries discussing the latest research, industry developments and clinical cases.
Professor Ian Morgan
BSc PhD
Research School of Biology, Australian National University, Canberra, ACT
Amanda French
BAppSci (Orth) Hons
Dr Kathryn Rose
GradDipNeurosci PhD
Discipline of Orthoptics, Graduate School of Health, University of Technology Sydney, Ultimo, NSW
Our new understanding of school myopia offers the realistic promise of effective control of progression of myopia, and some prospect of overall reductions in prevalence.
We have all used the term ‘school myopia,’ but often, it has been no more than a description of a condition that appears during the school years, along with the prevailing, if somewhat contradictory, belief that myopia was predominantly, if not exclusively, a genetic condition.¹
With the emergence of an epidemic of school myopia in East and Southeast Asia, a deeper understanding of school myopia has emerged over the past few years. There, the prevalence of school myopia has increased roughly three-fold over the last 50 years, with around 80 per cent of those completing 12 years of school now myopic (Figure 1). In the same parts of the world, the prevalence of high myopia (more severe than -6.00 D) has increased even more spectacularly (10–20-fold), with 10–20 per cent of students in their final years of schooling now highly myopic.² High myopia is generally associated with an increased risk of pathological myopia, which, in general, cannot be prevented or corrected by standard optical correction.³
Figure 1. In East Asia, around 80 per cent of those completing 12 years of school are myopic
These rapid changes are not consistent with the idea that school myopia is overwhelmingly genetically determined, since population gene pools cannot change that fast. Environmental factors must be involved. In a recent review, we have discussed in some detail why the debate in this area has been so confused.⁴
The two epidemics of myopia and high myopia are closely connected. In the current epidemic of myopia there has been an increasingly early onset of myopia, with over 50 per cent of children myopic by the end of primary school.⁵ A large proportion of children develop myopia at an age when progression is still rapid, with more time for progression before myopia stabilises late in the young adult years. Thus, an epidemic of myopia inevitably leads to an epidemic of high myopia, with increased loss of vision due to pathological myopia.
Environmental factors
Two environmental factors appear to play a major role in the emergence of the current epidemic.² The first is increased exposure to education. In the past, in societies where children received little formal education, the prevalence of myopia was only one to two per cent, most of which was probably genetic myopia. But as societies have developed more intensive mass education systems, the prevalence of school myopia has increased, no more so than in East and Southeast Asia.
The association between myopia and education is remarkably consistent, with children achieving higher school grades more likely to be more myopic.⁶ Similarly, in adults, final refraction is on average higher in those who have completed more years of schooling or achieved higher qualifications.⁷ But these associations do not establish causality, although some of the social correlations result from what are close to intervention trials. For the purists, the direction of causation, from education to myopia, has recently been demonstrated in a Mendelian randomisation study.⁸*
In parallel, children who spend more time outdoors are less likely to develop myopia. This is not a simple substitution effect, in which more time outdoors means less study, since the most at risk are children who combine lots of near work with little time outdoors, whereas children who combine lots of near work with lots of time outdoors are protected.⁹ Causality has been demonstrated in randomised school-based interventions,¹⁰ and the proposed causal mechanism, increased release of dopamine from the retina in the brighter light outdoors during daylight hours, has been confirmed in studies on experimental myopia.¹¹ The ‘high prevalence of myopia’ societies report much lower amounts of time spent outdoors by children than in western societies, where the prevalence of myopia is lower. Thus, it is likely that the epidemic of myopia in East and Southeast Asia results from a combination of intense education and limited time outdoors. It is currently unclear if time outdoors slows progression as well as onset, but marked seasonal effects on progression suggest that it might.
Prevention protocols
This new picture provides a clear link to prevention: through reducing educational pressures and increasing time outdoors. Reducing educational pressures may be difficult, given the importance of education in modern societies. However, it may be possible to modify some of the features of East Asian education that contribute to the development of myopia, such as the very early onset of educational pressures, with homework starting in pre-school, long school days with little time outdoors, heavy homework loads and extensive use of coaching classes. These features seem be related to intense competition for selective pathways that culminate in the final university entrance examination.
While change in these areas may be difficult, introducing more time outdoors into school programs is likely to be more feasible, provided that it does not intrude too much on the core business of education. Using existing optical, pharmacological and behavioural interventions for slowing myopia progression,¹² it should now be possible to nearly eliminate all but the clearly genetic forms of high myopia. Increased time outdoors is already a core part of national myopia prevention in Singapore and Taiwan, and is likely to have a significant part in mainland China’s developing myopia prevention protocols.
What does all this mean for Australia? In clinical practice, control of myopia progression now has to go hand in hand with correction. A number of optical and pharmacological approaches to prevention appear to work, but not all are strongly backed by evidence. Clinicians therefore need to investigate thoroughly the underlying evidence on the approaches they offer to clients. It also makes sense for clinicians to encourage more outdoor time, since myopia prevention does not appear to involve UV exposures and vitamin D levels, and is thus fully compatible with Australian skin protection policies.
One issue for the future is whether Australia will face increasing levels of myopia, as some modelling suggests. While there has been some increase in the prevalence of myopia in Australian children, this largely appears to be due to the increasing proportion of Australians of East Asian ancestry, who bring with them their cultural attitudes to education, and thus more myopia. In children of European ancestry, the prevalence of myopia is still under 20 per cent at the end of the school years (Figure 2). In those of East Asian ancestry, the prevalence of myopia may actually decline over time, if these communities increase engagement in outdoor activities, including sport. This development could be encouraged within schools.
Figure 2. The prevalence of myopia is still under 20 per cent for children of European ancestry at the end of their school years.
Other developments could, in contrast, lead to increases. In the past, we have heard repeated calls to adopt East Asian educational practices. In addition, there is increasing interest in the provision of universal pre-school education, to better prepare children from disadvantaged backgrounds for schooling. We need to ensure that this is delivered in a way that avoids the early onset of myopia now so common in East Asia. There is also considerable interest in the development of vertical pre-schools and schools. These could be a matter of concern, if they are designed in a way that limits student access to time outdoors.
Overall, the new understandings of school myopia offer the realistic promise of effective control of progression of myopia, and some prospect of overall reductions in prevalence. But at the same time, there are likely to be future challenges, and we need to keep an eye out for proposed changes in education that could compromise these advances.
*Footnote: Mendelian randomisation uses genetic variation as a natural experiment to investigate the causal relations between potentially modifiable risk factors and health outcomes in observational studies. The assumptions and limitations of the approach have been clearly reviewed.¹²³ In the case of myopia, genes associated with a small but measurable increase in years of schooling were also associated with increased myopia, where genes associated with a small increase in myopia were not associated with an increase in years of schooling.⁸
References
1. Sorsby A, Sheridan, M, Leary GA. Refraction and its components in twins. Special Reports Series of the Medical Research Council 1962; 303.
2. Morgan IG, French AN, Ashby RS et al. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res 2018; 62: 134-49.
3. Ohno-Matsui K, Lai TY, Lai CC et al. Updates of pathologic myopia. Prog Retin Eye Res 2016; 52: 156-87.
4. Morgan IG, Rose KA. Myopia: is the nature-nurture debate finally over? Clin Exp Optom 2019; 102: 3-17.
5. Lin LL, Shih YF, Hsiao CK et al. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore 2004; 33: 27-33.
6. Saw SM, Cheng A, Fonf A et al. School grades and myopia. Ophthal Physiol Optics 2007; 27: 126-9.
7. Mirshahi A, Ponto KA, Hoehn R et al. Myopia and level of education: results from the Gutenberg Health Study. Ophthalmology 2014; 121: 2047-52
8. Mountjoy E, Davies N, Plotnikov D et al. Education and myopia: a Mendelian randomisation study. BMJ 2018.
9. Rose KA, Morgan IG, Ip J et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 2008; 115: 1279-85.
10. He M, Xiang F, Zeng Y et al. Effect of Time Spent Outdoors at School on the Development of Myopia Among Children in China: A Randomized Clinical Trial. JAMA 2015; 314: 1142-8.
11. Ashby R, Ohlendorf A, Schaeffel F. The effect of ambient illuminance on the development of deprivation myopia in chicks. Invest Ophthalmol Vis Sci 2009; 50: 5348-54.
12. Huang J, Wen D, Wang Q et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology 2016; 123: 697-708.
13. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ 2018; 362: k601
Paediatric eye care reference guide
An outline of the components of a comprehensive vision and eye health examination for children, from birth to 14 years.
Reprinted from the 2019 Optometry Australia Clinical Practice Guide for paediatric optometry, this reference offers an overview of standard testing protocols by age, a guide to clinical normative values for accommodation and vergence parameters and average stereoacuity by age.
Dr Laura Downie
BOptom PhD(Melb) PGCertOcTher FAAO FACO DipMus(Prac) AMusA
Senior Lecturer, Department of Optometry and Vision Sciences, Faculty of Medicine, Dentistry and Health Sciences
The University of Melbourne
Clinical classifications, modifiable lifestyle factors and the quality of eye care
While therapeutic interventions exist for late-stage neovascular age-related macular degeneration (AMD), currently there are no approved medical therapies for earlier stages of the disease or late-stage geographic atrophy (GA). Given its association with sight-threatening retinal pathology, reducing progression to late-stage AMD is vital for decreasing vision loss and the associated individual and community burden of AMD.
AMD clinical classification
AMD is characterised by retinal changes that occur in a two-disc diameter radius of the fovea in people aged 55 years or older. The early stages of AMD are indicated by the appearance of drusen, comprising accumulations of lipoproteineous substance between the retinal pigment epithelium (RPE) and Bruch’s membrane. Drusen can also be associated with disruptions to the RPE, evident clinically as areas of relative hyper- or hypo-pigmentation. AMD can then progress to late-stage GA of the RPE and/or choroidal neovascularisation (CNV).
In 2013, the Beckman Initiative for Macular Research Classification Committee, a panel of international experts in the field, published a key paper defining an AMD clinical classification for implementation in clinical research and practice.¹ This classification system (summarised on pages 14 and 15 of the June issue of Pharma) defines five categories, based on retinal features, and is of value for predicting an individual’s risk of developing late-stage AMD.¹
There are several key points worth noting about this AMD classification scheme,² as follows:
AMD severity is described in three stages: ‘early,’ ‘intermediate’ and ‘late’
the terms ‘wet AMD’ and ‘dry AMD’ are not used in this classification. These descriptors were judged to be potentially confusing, as ‘dry AMD’ has historically been used to describe a spectrum of AMD-related changes, ranging from isolated drusen to GA
drusen are defined by their size (at their smallest diameter); subjective descriptors such as ‘soft’ and ‘hard,’ are not used
the presence of only drupelets (a small druse of less than 63 µm in diameter) within two-disc diameters of the fovea defines a pre-AMD category of ‘normal ageing changes,’ which is distinct from ‘early AMD.’
Risk factors for AMD
There are several risk factors for AMD. In terms of non-modifiable risk, advancing age is the strongest factor. The risk of developing AMD is three times higher in individuals older than 75 years, compared to those between 65 and 74 years of age.³ A family history of AMD, particularly having a first-degree family member affected by the condition, also confers a significantly-elevated risk of developing the disease.⁴ Of major clinical importance is identifying—and if possible modifying—lifestyle risk factors that can also influence the development and/or progression of AMD.
Tobacco smoking
Cigarette smoking is the single most important modifiable AMD risk factor;⁵ smoking at least doubles a person’s risk of developing the condition.⁶ Furthermore, a direct association has been identified between the number of cigarettes smoked over time and the risk of developing late-stage AMD.⁷ Despite these known links between tobacco smoking and sight-threatening ocular disease, studies suggest that primary eye care providers may not be routinely asking their patients about smoking or providing advice about the benefits of smoking cessation. Research undertaken in several developed countries,⁸-¹¹ including Australia,¹² involving surveys of eye care clinicians, identifies scope for optometrists to be more proactive in discussing tobacco smoking as a modifiable risk factor for eye disease with their patients. Eye care clinicians have identified a range of potential barriers to undertaking smoking counselling with their patients; these include a perceived lack of sufficient consulting time to perform this task, a perception that there should be sufficient public awareness about the health risks of smoking and/or considering discussing smoking habits with their patients to be too intrusive.¹²
With the intent of overcoming these barriers, and to assist eye care clinicians with capturing key information about a patient’s smoking behaviours and how these relate to AMD risk, my colleague Associate Professor Peter Keller and I developed a ‘Quantitative Clinical Smoking Behaviour Tool.’§ This tool, the first of its kind for eye-care clinicians, comprises 10 questions that capture information about a person’s smoking behaviours, across three main areas:
Current and former smoking status (using a validated classification system), and how this informs a person’s risk of developing AMD or having progressive disease.
Degree of smoking dependence, which relates to a current smoker’s level of nicotine dependence.
Level of motivation to cease smoking, to ascertain a current smoker’s readiness to consider smoking cessation, quantified on a validated behavioural scale.
For each of these three key areas, the tool provides an evidence-based summary (including a comprehensive list of relevant citations) that eye care clinicians can use to provide evidence-based advice to patients about the benefits of smoking cessation for their eye health.
Diet
Diet is another key area for potential AMD risk modification. Multiple epidemiological studies have reported the potential benefits of a healthy diet, rich in the macular carotenoids (zeaxanthin and lutein) and omega-3 fatty acids, for lowering the risk of developing AMD. A meta-analysis that included several observational studies reported that the consumption of two or more servings of oily fish per week was beneficial in the primary prevention of AMD.¹³
High glycaemic index diets and alcohol consumption (in excess of two drinks per day) may also increase the risk of AMD, although further studies are required to confirm these associations.¹⁴
A recent systematic review concluded that high consumption of vegetables rich in carotenoids and oily fish containing omega-3 fatty acids was beneficial for people at risk of AMD.¹⁴ However, emphasising the need to differentiate between nutritional components derived from whole foods and supplementation, consuming anti-oxidant supplements does not prevent the development of AMD.¹⁵
In terms of modifying AMD progression, a Mediterranean diet (rich in foods such as fruits, vegetables, legumes, and fish) has been linked to a reduced risk of AMD progression.¹⁶ Epidemiology studies suggest that a high dietary intake of omega-3 fatty acids is associated with a significant reduction in the risk of both intermediate¹⁷,¹⁸ and late-stage AMD.¹⁹,²⁰ It has also been recommended that vegetable oils and animal fats (which contain high levels of omega-6 fatty acids) and red/processed meat should be consumed minimally to reduce the risk of AMD progression.¹⁴
Supplements
With respect to supplementation, the Age Related Eye Disease Study (AREDS) showed that daily, long-term, high-dose supplementation with vitamin C (500 mg), vitamin E (400 IU), beta-carotene (15 mg), zinc (80 mg, as zinc oxide), and copper (2 mg, as cupric oxide) in people with at least intermediate-stage AMD reduced the relative risk of progression to late AMD from 28 per cent to 20 per cent at five years.²¹ As such, it may be relevant to consider the potential benefit of a high-dose anti-oxidant vitamin and mineral supplement in individuals with intermediate-stage AMD. The decision to recommend such formulations to patients requires consideration of the patient’s systemic health, as well as the relative benefits versus risks of supplementation. For example, there is evidence that the risk of lung cancer is significantly increased with high-dose beta-carotene supplementation in current and former smokers.²²,²³
A quantitative clinical diet and nutritional supplement tool§ is also now available for optometrists to use in their practice. This simple survey, developed as a companion to the smoking behaviour tool, supports the capture of key clinical information relating to an individual’s diet that are relevant to the risk of AMD, as follows:
omega-3 fatty acid intake
lutein and zeaxanthin intake
nutritional supplement consumption.
Clinical audit
The MaD-CCAT tool
Through a collaborative project with Professor Robyn Guymer, Associate Professor Peter Keller, Dr Lauren Ayton, Professor Algis Vingrys and Ms Ji-hyun (Anna) Lee, funded by the Macular Disease Foundation Australia, my research team has developed an optometric clinical audit tool for assessing the quality of eye care provided to people with AMD.
The MaD-CCAT tool enables optometrists to evaluate their practices with respect to the clinical care provided to their AMD patients, relative to current evidence-based standards. This process enables the identification of potential areas for practice improvement, to enhance the quality and outcomes of optometric patient care to people with AMD.
The MaD-CCAT supports streamlined auditing of multiple aspects of AMD clinical care, including: the identification of modifiable risk factors, diagnostic accuracy (including AMD severity classification), rate/timeliness and appropriateness of referrals for ophthalmologic evaluation, and the quality of clinical record keeping.
Data are captured using a check-box system, for ease of entry. A summary statistics worksheet then automatically populates information comparing an optometrist’s practices with current best-practice guidelines for diagnosing and managing AMD.
A representative snapshot of the data analytics ‘Overview’ page is provided in Figure 1. As audit data are progressively added, the summary statistics highlight areas of relative strength and potential areas for practice improvement. Clinicians can then self-identify practice areas for continuous improvement.
It is of vital importance that primary eye-care providers identify and provide evidence-based advice to their patients in relation to modifiable risk factors for AMD. The availability of new clinical tools to enable clinicians to undertake these assessments, and self-evaluate their own clinical practices, provides a basis for ongoing practice improvement to optimise the delivery of primary eye care to people with AMD.
Figure 1. Snapshot of the MaD-CCAT analytics page, which provides clinicians with summarised information about their clinical audit contributions.
References
1. Ferris FI, Wilkinson CP, Bird A et al. Clinical Classification of Age-related Macular Degeneration. Ophthalmology 2013; 120: 844-851.
2. Downie LE, Keller PR. Nutrition and age-related macular degeneration: research evidence in practice. Optom Vis Sci 2014; 91: 821-831.
3. Klein R KB, Knudtson MD, Meuer SM et al. Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study. Ophthalmology 2007; 114: 253-262.
4. Klein ML, Francis PJ, Ferris FL, 3rd et al. Risk assessment model for development of advanced age-related macular degeneration. Arch Ophthalmol 2011; 129: 1543-1550.
5. Thornton J, Edwards R, Mitchell P et al. Smoking and age-related macular degeneration: a review of association. Eye (Lond) 2005; 19: 935-944.
6. Evans JA, Fletcher AE, Wormald RP. 28,000 Cases of age related macular degeneration causing visual loss in people aged 75 years and above in the United Kingdom may be attributable to smoking. Br J Ophthalmol 2005; 89: 550-553.
7. Khan JC, Thurlby DA et al. Smoking and age related macular degeneration: the number of pack years of cigarette smoking is a major determinant of risk for both geographic atrophy and choroidal neovascularisation. Br J Ophthalmol 2006; 90: 75-80.
8. Lawrenson JG, Evans JR. Advice about diet and smoking for people with or at risk of age-related macular degeneration: a cross-sectional survey of eye care professionals in the UK. BMC Public Health 2013; 13: 564.
9. Thompson C, Harrison RA, Wilkinson SC et al. Attitudes of community optometrists to smoking cessation: an untapped opportunity overlooked? Ophthal Physiol Opt 2007; 27: 389-393.
10. Caban-Martinez AJ, Davila EP, Lam BL et al. Age-Related Macular Degeneration and Smoking Cessation Advice by Eye Care Providers: A Pilot Study. Prev Chron Dis 2011; 8: A147.
11. Brûlé J, Abboud C, Deschambault E. Smoking cessation counselling practices among Québec optometrists: evaluating beliefs, practices, barriers and needs. Clin Exp Optom 2012; 95: 599-605.
12. Downie LE, Keller PR. The self-reported clinical practice behaviors of Australian optometrists as related to smoking, diet and nutritional supplementation. PLOS One 2015.
13. Chong EW, Wong TY, Kreis AJ et al. Dietary antioxidants and primary prevention of age related macular degeneration: systematic review and meta-analysis. BMJ 2007; 335: 755.
14. Chapman NA, Jacobs RJ, Braakhuis AJ. Role of diet and food intake in age-related macular degeneration: a systematic review. Clin Exp Ophthalmol 2019; 47: 106-127.
15. Evans JR, Lawrenson JG. Antioxidant vitamin and mineral supplements for preventing age-related macular degeneration. Cochrane Database Syst Rev 2017; 7: Cd000253.
16. Merle BMJ, Colijn JM, Cougnard-Gregoire A et al. Mediterranean Diet and Incidence of Advanced Age-Related Macular Degeneration: The EYE-RISK Consortium. Ophthalmology 2019; 126: 381-390.
17. Christen WG, Schaumberg DA, Glynn RJ et al. Dietary omega-3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch Ophthalmol 2011; 129: 921-929.
18. Seddon JM, George S, Rosner B. Cigarette smoking, fish consumption, omega-3 fatty acid intake, and associations with age-related macular degeneration: the US Twin Study of Age-Related Macular Degeneration. Arch Ophthalmol 2006; 124: 995-1001.
19. Chong EW, Kreis AJ, Wong TY et al. Dietary omega-3 fatty acid and fish intake in the primary prevention of age-related macular degeneration: a systematic review and meta-analysis. Arch Ophthalmol 2008; 126: 826-833.
20. Sangiovanni JP, Agron E, Meleth AD et al. {omega}-3 Long-chain polyunsaturated fatty acid intake and 12-y incidence of neovascular age-related macular degeneration and central geographic atrophy: AREDS report 30, a prospective cohort study from the Age-Related Eye Disease Study. Am J Clin Nutr 2009; 90: 1601-1607.
21. Age-related eye disease study research group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001; 119: 1417-1436.
22. The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med 1994; 330: 1029-1035.
23. Omenn GS, Goodman GE, Thornquist MD et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med 1996; 334: 1150-1155.
§ Optometrists interested in accessing the MaD-CCAT tool, the diet and nutritional supplement tool and the quantitative clinical smoking behaviour tool can email the author directly at l.downie@unimelb.edu.au
Anti-VEGF injections and the prevention of irreversible visual loss
Dr Simon Chen
MBBS (London), BSc (Hons)
FRCOphth FRANZCO
Retinal & Cataract Surgeon
Conjoint Senior Lecturer, University of NSW
Kerryn Hart
BOptom GCertOcTher MPH
Clinical Skills Teacher In Optometry, Deakin University
Optometry Australia Policy and Standards Advisor
Clinical Editor of Pharma
The role of the optometrist in improving patient adherence to therapy
Anti-vascular endothelial growth factor (anti-VEGF) drugs have revolutionised the treatment of age-related macular degeneration (AMD) and have preserved the vision of patients throughout the world. Still, many millions remain at risk of severe AMD-related vision loss, and perhaps most disconcertingly, it is because they have chosen to discontinue their treatment.
Pharma’s Clinical Editor Kerryn Hart recently conducted an interview with retinal surgeon Simon Chen to discuss the burdens and benefits of intravitreal injections and the role of the optometrist in improving patient adherence to anti-VEGF therapy. An edited version of the interview appears below.
KH: Dr Chen, anti-VEGF therapy has been an established treatment for neovascular AMD (nAMD) since 2006. Has anything changed since its initial appearance?
SC: The treatment itself has not fundamentally changed, the anti-VEGF agent is administered into the eye via an intravitreal injection on a regular basis. Beyond that, there have been three fundamental changes: 1) there has been a movement toward customised treat-and-extend protocols; 2) a growing understanding of the importance of aggressive and long-term treatment of nAMD; and 3) since 2006, a wider range of anti-VEGF agents have become available.
Undeniably, we now have a much greater understanding of important aspects of anti-VEGF therapy such as the pros and cons of different treatment regimens, the importance of life-long treatment for most patients, the risks and benefits of treatment and the long term visual outcomes of therapy.
Treat and extend protocols
Retinal specialists are shifting away from pro re data (PRN) treatment protocols (where injections are only administered when signs of disease activity recur) and regular fixed interval treatment protocols (where all patients are injected every four weeks) and towards customised ‘treat and extend’ protocols whereby the frequency of injections is tailored to the individual patient according to their own response to treatment.
Treat and extend protocols have been shown to provide better visual results than PRN protocols while reducing the number of injections needed compared to regular fixed interval treatment protocols.¹
Importance of aggressive and long-term treatment
It’s now well-established that patients need to be treated early in the disease process (that is, as soon as signs of nAMD become apparent). Treatment also needs to be administered frequently, especially in the early stages, when the disease is most active. We now know that for the majority of patients with nAMD, long term, potentially life long, anti-VEGF treatment is required because high rates of disease reactivation and permanent visual loss have been reported in patients that cease therapy.
KH: I’ve read that patients are often lost to follow-up with their anti-VEGF regime. Does your experience show this?
SC: Recent studies in the United States have indicated that up to 25 per cent of patients that start anti-VEGF treatment are eventually lost to follow-up.² This figure, of course, varies significantly between ophthalmic practices due to differences in patient demographics (older patients may find it more difficult logistically to attend for treatment and may be limited by other co-morbidities), patient socio-economic status and geographic location of the clinic.
KH: What are the key factors for patient drop out?
SC: For new patients, fear about possible pain or complications associated with the injection procedure are a common and natural reaction, especially in patients with a tendency towards anxiety.
Logistic barriers are a common cause for patients to drop out of treatment. (Difficulties travelling to and from a clinic due to factors such as inability to drive, difficulties accessing public transport, limited wheel chair access, poor memory causing patients to forget appointments, the need to arrange carers who may need to take time off work for injection visits). Patients may experience guilt about the ongoing burden on carers which in turn may makes them less likely to attend for treatment.
In older patients, co-morbidities may limit their access to care. For example: a patient suffering a hip fracture may be hospitalised and require long-periods of post-op rehabilitation causing them to miss out on scheduled anti-VEGF injections.
For patients with financial difficulties, concerns about out-of-pocket-costs associated with treatment may impact their treatment decision. Over time, ‘injection fatigue’ can set in among patients as they become frustrated with the ongoing need for treatment causing their commitment to treatment to wane.
For some patients there may be a lack of perceived benefit especially if treatment has not led to an improvement in their vision or their vision has continued to deteriorate despite treatment.
KH: What role does the optometrist play in improving compliance with anti-VEGF injections?
SC: Optometrists have a vital role to play in optimising patients’ compliance with anti-VEGF therapy and therefore maximising their visual function and quality of life.
They can do this at an early stage by educating their patients with early-to-intermediate AMD about the long term risk of developing the neovascular form of AMD and making them aware of the potential vision-saving benefits of anti-VEGF injections before they have even developed nAMD. By exposing patients to the notion that anti-VEGF injections are an important treatment at an early stage, they may be better primed to accept the need for treatment when the time comes.
When optometrists refer patients with neovascular AMD to an ophthalmologist for anti-VEGF treatment, they can facilitate patient compliance by stressing the importance of attending the appointment without unnecessary delay. This should involve explicitly telling the patient that they are at risk of permanent visual loss if their condition is not assessed and managed in an appropriately urgent time frame. Without this information being provided to them, patients may not always appreciate the urgency of initiating treatment and so may delay seeing an ophthalmologist, potentially leading to irreversible visual loss due to progression of the neovascular process.
Optometrists also have an important continuing role in supporting patient compliance throughout the course of ongoing anti-VEGF therapy by providing ongoing educational and sometimes even emotional support. Patients should be reminded about the importance of ongoing treatment at every eye examination.
Many patients and their carers do not realise that nAMD is a chronic disease which is likely to require life-long treatment and unless patients are treated aggressively, they will generally lose vision. Real-world evidence has shown that anti-VEGF injection frequency is an important factor in achieving optimal gains in vision. In Australia, the Fight Retinal Blindness Study Group reported that visual acuity was maintained throughout five years of anti-VEGF treatment.³ On average patients receive about five injections per year. Despite this, relative under-treatment is common.
Consistent messaging from different health care providers, including ophthalmologists, optometrists and general practitioners, helps to maintain patient compliance with treatment.
Patients should be encouraged to continue having regular optometric reviews even when they are having regular anti-VEGF injections as it is important that patients have the best optical correction possible in order to maximise their limited vision. Optometrists are well positioned to detect interval ocular pathology such as cataracts and assess the potential need for low vision services in patients with reduced vision.
Some patients are reluctant to voice concerns with their ophthalmologist and feel more comfortable discussing them with their optometrist. Concerns about injection-related discomfort, clinic waiting times and out-of-pocket costs are examples of issues that patients may find easier discussing with their optometrist. By encouraging the patient to talk to their ophthalmologist or liaising with the ophthalmologist on behalf of the patient, these issues can be addressed and optometrists may potentially prevent patients being lost to follow-up.
KH: Can you give any examples of where the optometrist has played an important role in improving/maintaining compliance with anti-VEGF injections?
SC: One example I am often reminded of is that of an 85 year-old woman that I am still seeing for regular anti-VEGF injections. She is an avid reader and passionate about painting. She is fiercely independent. Approximately five years ago, she developed loss of central vision in her only seeing eye. The fellow eye had become blind following complications of cataract surgery. Her vision had deteriorated rapidly to 6/60 over the course of a week due to nAMD. She had lost the ability to read, paint and drive. She was distressed about the possibility of losing her independence as she lived alone. She was referred to me for assessment by her optometrist whom she had been seeing for approximately 20 years.
At the initial consultation, I confirmed a diagnosis of nAMD and urged her to have treatment with anti-VEGF injections the same day. Despite my best efforts, she refused treatment because of a fear of complications that might lead to her losing more vision, as had happened when she had previously had cataract surgery. She promised to return the next day for treatment after she had time to collect her thoughts. The next day she failed to attend our arranged appointment and treatment. I spoke with her on the phone and she stated that she had determined that she did not want treatment and would just take her chances, letting nature take its course.
I called to explain the situation to her optometrist who took quick action in calling her and managed to convince her to attend for treatment the same day. It was the long-term rapport that she had built up with her optometrist over the years that provided the confidence to trust his advice. He explained that we had shared numerous patients with nAMD together and that the results had been very positive. He reiterated the potential consequences on her quality of life of not having treatment. She responded extremely well to treatment, eventually regaining a visual acuity of 6/9 which has been maintained to this day. She remains fully independent and her passion for reading and painting is unchanged.
Figure 1. The intravitreal injection procedure. Images courtesy of Novartis.
KH: What happens to our (optometrists’) patients when they come for anti-VEGF injections? That is: what is the procedure they can expect to go through?
SC: Following referral of a patient with nAMD by an optometrist for anti-VEGF injections, patients can expect to consult with an ophthalmologist. A typical initial consultation will involve history taking, dilated clinical examination and retinal imaging with fundus photography and optical coherence tomography (OCT) scanning. Additional retinal imaging tests such as OCT-angiography, fluorescein angiography, indocyanine green angiography or fungus autofluorescence may also be performed to confirm a diagnosis of nAMD.
Once a diagnosis of nAMD has been confirmed a decision will be made regarding whether that patient may benefit from anti-VEGF therapy. A minority of patients may not benefit if their condition is too far advanced and they have evidence of severe permanent macular scarring. Assuming that anti-VEGF therapy is indicated, then the pros and cons of treatment will be discussed with the patient and they will be informed about the potential and likely need for long-term therapy. The initial anti-VEGF injection should be performed as soon after diagnosis as practical to avoid the potential for on-going visual loss to occur. Many ophthalmologists will initiate treatment at the first visit or within a few days of the initial visit. Treatment may be performed in the ophthalmologist’s clinic room, a dedicated treatment room in the clinic or in a day surgery setting.
The technical aspects of the injection can vary widely between ophthalmologists (the type of anaesthesia used, the type of antiseptic agent, whether or not a lid speculum is used, the use of post-injections drops) which can cause the patient experience to vary significantly between different ophthalmologists. However, the fundamental steps of the injection will always include the application of some form of ocular anaesthetic (drops, gel or subconjunctival injection) and topical antisepsis (with povidone iodine or chlorhexidine) followed by the intravitreal injection of anti-VEGF agent via a needle passed through the pars plana. Depending on the treating ophthalmologist’s preference, patients may be advised to use drops (lubricants, steroids or antibiotics) following the injection. Some ophthalmologists tend to treat both eyes of patients with bilateral nAMD on the same day, while others may prefer to treat each eye on different days.
Following the initial injection, patients may be reviewed anytime from within a few days after the injection to four weeks later. Patients are typically scheduled to have the second anti-VEGF injection four weeks after the first.
When the patient presents for the second injection, they will be clinically assessed to check their visual acuity and intraocular pressure. The ophthalmologist may perform a clinical exam and/or OCT scan to assess disease activity.
KH: What happens after the procedure?
SC: Depending on the routine of the treating ophthalmologist preference, some patients may have their treated eye covered by an eye pad or shield. They may be advised to use drops after the injection including lubricants, steroids or antibiotics. The trend is increasingly for no post-injection antibiotics to be prescribed due to evidence showing that they do not reduce endophthalmitis rates and concerns that their routine use may promote antibiotic resistance.
Generally, patients should not drive immediately after an injection.
It is common to experience minor dry eye symptoms secondary to the use of topical anaesthetic and antiseptic used during the procedure. These symptoms will usually resolve completely by the next morning but may occasionally persist for up to 72 hours.
KH: Many patients are worried that anti-VEGF treatment will be painful. What can we tell them?
SC: Patients should be reassured that it is a very natural response to worry that anti-VEGF injections may be painful. Although patients may experience minor discomfort during the injection process, the large majority of patients do not experience significant pain at any stage and most patients experience no pain at all at any stage.
Ophthalmologists experienced in administering anti-VEGF injections have typically performed many hundreds if not thousands of injections enabling them to hone their techniques to minimise pain and discomfort.
Having said that, a minority of patients may experience pain associated with an injection. There are many technical nuances to performing intravitral anti-VEGF injections that can have a large impact on patient comfort during or after an injection. It is important for patients to know that if they do have a painful experience, they should inform their ophthalmologist so that they can make amendments to the injection technique for the next injection. Different patients may respond quite differently to the same technique. For example: some patients find the use of povidone iodine causes severe pain whereas other patients may not, so in such a patient, switching the antiseptic used to chlorhexidine may enable a pain-free experience.
Patients should be informed that if they do experience pain during treatment, the pain is usually very brief and can be managed appropriately. Reminding the patient that the bigger picture is that the injections are important to optimise the patient’s vision and ultimately their quality of life and independence.
KH: What is the risk of serious complications?
SC: Fortunately, the risk of serious vision-threatening complications with anti-VEGF injections is low. Possible sight-threatening complications can occur and include:
endophthalmitis reported to occur at a rate between 0.019% and 0.09%. Many cases of endophthalmitis can be successfully treated with recovery of good levels of visual acuity but some cases may not respond as well ultimately leading to permanent loss of vision.
retinal detachment (under 0.05%)
cataract due to the needle used to inject the anti-VEGF agent inadvertently touching the crystalline lens
KH: What are the potential side effects?
SC: A number of non-sight threatening side effects may commonly occur, including:
subconjunctival haemorrhage which is common but harmless although it may be a cosmetic concern for some patients. It will typically resolve within 14 days.
dry irritable eye, transient floaters and transient blurring of vision immediately after the injection which usually resolve by the next day.
References
1. Mantel I. Optimizing the Anti-VEGF Treatment Strategy for Neovascular Age-Related Macular Degeneration: From Clinical Trials to Real-Life Requirements. Transl Vis Sci Technol. 2015; 4: 6.
2. Weiss M, Sim D, Herold T et al. Compliance and adherence of patients with diabetic macular edema to intravitreal anti-vascular endothelial growth factor therapy in daily practice. Retina 2018; 38: 2293–300.
3. Gillies MC, Campain A, Barthelmes D et al. Long-Term Outcomes of Treatment of Neovascular Age-Related Macular Degeneration: Data from an Observational Study. Ophthalmology. 2015; 122: 1837-1845
Clinical classification for Aged-Related Macular Degeneration (AMD)
Clinical classification for AMD
Reprinted from the 2019 Optometry Australia Clinical Practice Guide for the diagnosis, treatment and management of AMD, the Beckman classification offers a guide to identify normal, early, intermediate and late AMD.
Dr Angelica Ly PhD GradCertOcTher BOptom (Hons) FAAO
Integrated Care Co-ordinator and Lead Clinician (macula)
Centre for Eye Health
Age-related macular degeneration (AMD) is the leading cause of vision loss and blindness in Australia.
One in four cases of AMD are classified as normal by eye care professionals.1 Poor visual acuity at presentation translates to poor outcomes and up to 87 per cent of patients with neovascular AMD have a visual acuity worse than 6/12 at the time of diagnosis.²,³ Additionally, one in five patients that need treatment may be lost to follow-up.⁴
These statistics paint a sobering picture on the state of AMD care in Australia and worldwide. In this article, I describe a series of clinical strategies to supercharge the way you diagnose, understand and manage AMD.
Confession 1: The rules keep changing
Solution: Clinical practice guidelines
There is a plethora of resources now available to practising clinicians aimed at improving clinical practice patterns and ultimately, patient outcomes. Broadly, these resources include convenient and easily-accessible forms of information, such as case studies, peer-reviewed publications, chair-side references and clinical guidelines (Table 1).⁵
Optometry Australia has recently developed a clinical practice guide, providing evidence-based information about current best practice in the diagnosis, treatment and management of age-related macular degeneration. This is an open-access resource available on the Optometry Australia website.
Because the collective wisdom is constantly evolving, these tools can be helpful for distinguishing fact from fiction and often provide all of the relevant information succinctly, filtered through the lens of an expert committee. Although the evidence for efficacy of these materials is limited and the best approach for optimising their efficacy still requires clarification, they are indeed one of the few methods we have of translating research findings into clinical practice. They help to define and promote the use of evidence-based procedures of proven benefit and discourage ineffective alternatives.
In these materials, you can find ready support on a myriad of topics ranging from general management advice, diagnosis, procedures, referrals, test ordering, patient education, clinical prevention and professional-patient communication. They may be accessible through one or multiple means (either personally, online, through mass mailing and most commonly, via publication in a peer-reviewed journal) and result in a statistically significant improvement in professional practice.⁵
Confession 2: I am not confident about what I’m seeing
Solution: Clinical decision support platforms
Today’s ‘routine’ eye examination is incredibly complex. In AMD alone, we may be accustomed to performing a targeted history, a routine battery of entrance tests, followed by fundoscopy and retinal photography. It helps to know which instrument to use and when. Optical coherence tomography (OCT) is quickly becoming the norm⁶ and OCT angiography, fundus autofluorescence and other imaging techniques, including near infrared imaging or ultra-widefield imaging, are also effective.⁷,⁸ The combination of multiple modalities improves the diagnosis of ocular disease but may not always be accessible and is often time consuming and subject to interpretation.
Take for instance, a routine 512 x 128 macular OCT volume scan acquired using the Cirrus HD-OCT (Carl Zeiss Meditec). This means that in addition to the rest of the examination, the optometrist has an added duty of care to review each of the 128 serial line scans taken per eye, meaning a total of 256 B-scans per patient. Add to this the myriad of prognostic biomarkers, which are relevant to stratifying risk of AMD progression⁹ and the complexity is mind-boggling.
Support for accurately interpreting imaging results is on its way. With the aid of computational approaches and machine learning, we can expect to see a growing suite of clinical decision-making support tools. Risk calculators represent an example many will be more familiar with, which is commonly applied to case history data.
Figures 1 and 2 showcase two computational methods of analysing AMD-related ocular imaging data in development at the Centre for Eye Health.¹⁰,¹¹ Current commercially-available software on the Cirrus HD-OCT, described as ‘advanced retinal pigment epithelium (RPE) analysis,’ presents a similar tool with the capacity to automatically quantify drusen load.
Figure 1. A clinical decision support tool currently in development at Centre for Eye Health. This method uses unsupervised cluster analysis to semi-automatically classify drusen (red) and pigmentary abnormalities (blue). Each distinct colour in the profile map corresponds to a statistically separable, specific anatomic structure.
Figure 2. Case images taken 16 months apart from an eye with intermediate AMD. The change or difference map pictured on the right alerts the clinician to areas of drusen regression (red).
Confession 3: My patients refuse to quit smoking
Solution: Motivational interviewing and printed patient educational materials
Having fulfilled the onerous task of keeping up-to-date with the latest evidence, acquiring and correctly interpreting the sum of results from the eye examination, it can be tempting to presume that our job is done; however, all that work may be in vain if not disseminated to the patient. Several risk factors carry a well-described association with the onset and progression of AMD, such as age, family history and smoking. Hypertension, cardiovascular disease, raised BMI, poor diet and lack of exercise are less often considered but represent additional and more importantly, modifiable risk factors for disease. Therefore, your AMD management strategy should regularly include advice on improving dietary habits as well as the benefits of nutritional supplements and quitting or reducing smoking.
As optometrists, our unique position in the health care system empowers us to educate and reinforce key management strategies that can make a difference and ultimately, save sight. Behaviour change in chronic disease can be difficult, particularly in asymptomatic cases where the fear of change, ambivalence, lack of skills or a history of prior failures abound; however, it can also be one of the most rewarding aspects of routine optometric practice and a real relationship-builder between you and your patients.
I encourage you to have those ‘difficult’ conversations. But be advised that authoritarian, confrontational or guilt-inducing communications are often counter-productive. If you’re finding it hard to know where to start, motivational interviewing describes an evidence-based, directive counselling approach to behaviour change. I urge all practitioners to learn more about its application in chronic diseases.¹² Personalising the message to the individual is important and relevant material or contact from patient support groups, such as the Macular Disease Foundation Australia, or low vision services, including Guide Dogs Australia or Vision Australia, can also be invaluable.
Optometry has entered a period with an ever-increasing range of tools and information to supercharge the way we manage AMD and other diseases. With this comes both challenges and opportunities to apply strategies for the benefit of our patients. How will you improve the way you manage AMD tomorrow?
Conflicts of interest: The author is a named inventor on a provisional patent relating to the use of pattern recognition on ocular imaging data. Centre for Eye Health is an initiative of Guide Dogs NSW/ACT and UNSW Sydney and has an affiliation with the Macular Disease Foundation Australia.
Acknowledgements: The author thanks Michael Yapp and Professor Michael Kalloniatis for reviewing the manuscript.
References
1. Neely DC, Bray KJ, Huisingh CE et al. Prevalence of Undiagnosed Age-Related Macular Degeneration in Primary Eye Care. JAMA Ophthalmol 2017; 135: 570-575.
2. Fong DS, Custis P, Howes J et al. Intravitreal bevacizumab and ranibizumab for age-related macular degeneration a multicenter, retrospective study. Ophthalmology 2010; 117: 298-302.
3. Ho AC, Albini TA, Brown DM et al. The Potential Importance of Detection of Neovascular Age-Related Macular Degeneration When Visual Acuity Is Relatively Good. JAMA Ophthalmol 2017; 135: 268-273.
4. Obeid A, Gao X, Ali FS et al. Loss to Follow-up Among Patients With Neovascular Age-Related Macular Degeneration Who Received Intravitreal Anti-Vascular Endothelial Growth Factor Injections. JAMA Ophthalmol 2018; 136: 1251-1259.
5. Giguere A, Legare F, Grimshaw J et al. Printed educational materials: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev 2012; 10: CD004398.
6. Ly A, Nivison-Smith L, Zangerl B et al. Self-reported optometric practise patterns in age-related macular degeneration. Clin Exp Optom 2017; 100: 718-728.
7. Ly A, Nivison-Smith L, Assaad N et al. Infrared reflectance imaging in age-related macular degeneration. Ophthalmic Physiol Opt 2016; 36: 303-316.
8. Ly A, Nivison-Smith L, Assaad N et al. Fundus Autofluorescence in Age-related Macular Degeneration. Optom Vis Sci 2017; 94: 246-259.
9. Ly A, Yapp M, Nivison-Smith L et al. Developing prognostic biomarkers in intermediate age-related macular degeneration: their clinical use in predicting progression. Clin Exp Optom 2018; 101: 172-181.
10. Ly A, Nivison-Smith L, Assaad N et al. Multispectral Pattern Recognition Reveals a Diversity of Clinical Signs in Intermediate Age-Related Macular Degeneration. Invest Ophthalmol Vis Sci 2018; 59: 1790-1799.
11. Ly A, Yapp M, Kalloniatis M, Zangerl B. Automated identification of drusen regression. American Academy of Optometry Annual meeting, San Antonio, Texas, 2018.
12. Linden A, Butterworth SW, Prochaska JO. Motivational interviewing-based health coaching as a chronic care intervention. J Eval Clin Pract 2010; 16: 166-174
Mistakes not to make in glaucoma management
Dr Joseph Sowka
OD FAAO Diplomate
Nova Southeastern University
College of Optometry
Ft. Lauderdale, FL, USA
Diagnosing and managing patients with glaucoma can be a challenging task.
Glaucoma can be diagnosed by observations of characteristic changes in the optic disc and retinal nerve fibre layer (RNFL), abnormalities in threshold perimetry, alterations in structure demonstrated on optical coherence tomography (OCT) and assessment of risk factors such as intraocular pressure (IOP) and family history of the disease.¹ Therapeutic intervention is generally straightforward; that is, reduction of IOP with medicines, lasers and/or surgery. However, errors in diagnosis and therapeutics can make glaucoma management an arduous task. Take care not to make these common errors
Mistake #1: Not recognising when the OCT is wrong
There are several issues in imaging that make OCT assessments for glaucoma very suspect and even misleading. A relatively limited normative database (against which the patient’s measurements are compared), signal quality, blinks and saccades, segmentation errors, media opacities and an abnormal axial length can all contribute to induced false measurements on an OCT.
When interpreting an OCT printout, ensure that the quality score (as indicated for each specific proprietary device) has been met at a minimum. Look to see that there is proper illumination and clarity of focus and the optic disc image is properly centred with no missing data. Inspect the scan for signs of eye movement. Look to see how the device has segmented the individual layers to ensure that no artificial errors have been introduced. Posterior vitreous detachments and other vitreal issues may confuse the device and make it seem that it is measuring tissue that isn’t really there. Finally, if using any macular scans or ganglion cell analysis measurements, ensure that there is no concurrent macular disease. If there is, then do not use this potentially misleading information.²-⁴ (Figures 1 and 2.)
Figure 1. Abnormal OCT due to missing data from blink. Note how the RNFL thickness superiorly drops to ‘0.’ This never happens anatomically and is a result of the missing data rather than true glaucomatous loss.
Figure 2. Abnormal ganglion cell analysis OS due to epiretinal membrane and macular pseudo-hole. Such images of concurrent disease should not be used in glaucoma analyses.
Mistake #2: Treating ‘red disease’
Most OCT printouts colour-code results as to degree of statistical significance. Common coding uses green to connote the patient’s measured data to be within 95 per cent confidence intervals, red to indicate when findings would occur normally in just one per cent of the population, and yellow to indicate all intervening values with borderline significance. In that each OCT manufacturer employs a relatively limited normative database to compare against, there commonly will be situations where a patient’s measured data falls outside the device’s normative database, yet the patient may be completely healthy and normal. Just because a patient’s measured information falls outside the 99 per cent level doesn’t mean that there is disease present. In this instance, much of the printout will be coded as abnormal in red, yet there is truly no disease present. This is commonly referred to as ‘red disease.’⁵
The use and overemphasis of imaging technology to the exclusion of additional clinical findings and assessment of risk will put patients in peril. All imaging technology must be interpreted in context with other clinical findings and when the OCT results do not fit with known correlates of glaucoma, the results should be interpreted with caution (Figure 3).
Figure 3. Left superior temporal OCT abnormality in an eye with a robust OCT thickness map, normal visual field, and ophthalmoscopically normal optic disc and RNFL as an example of ‘red disease’
Mistake #3: Not treating ‘real disease’
Similar to red disease discussed above, there may be instances where patient data may fall within the OCT normative confidence interval with results printed in green, yet have clinically, ophthalmoscopically visible damage to the RNFL and functional loss on threshold perimetry.⁶ This commonly occurs when inspecting the quadrant and clock hour graphs on OCT. When the RNFL analysis is divided into four quadrants or 12 clock hours, it must be remembered that considerable area is being averaged to give these sector values. A focal RNFL defect may be present ophthalmoscopically, but when averaged in with adjacent healthy tissue on OCT, the value may fall within the device’s normative database. Thus, everything is printed in green, giving a false sense of security in an eye that truly has structural damage. Thus, it is important to weigh the OCT results against the optic disc photographs and clinical examination to ensure that “green disease” is not missed⁷ (Figure 4).
Figures 4. A: An ophthalmoscopically visible RNFL defect. B: A normal OCT with all data falling within the device’s normative database in a classic example of ‘green disease.’
Mistake #4: Changing therapy based upon one bad IOP reading or one changed visual field
Intraocular pressure measurements and visual field results can be variable, especially when one considers patient compliance with medications and the psychophysical responses in threshold perimetry. Patients often overstate adherence to medical therapy. Even when not trying to be intentionally misleading, many patients may not correctly remember if they used their medication properly immediately before the examination. Medicines don’t fail overnight. A medically adherent patient will not have an IOP of 15 mmHg on one visit and 30 mmHg on the next visit due to medicine failure or progressing trabecular dysfunction.
There will be a slow, progressive upward drift of IOP in cases where medicines are failing to control IOP. Always insist at least two IOP readings above target (and preferably three) before making any therapeutic changes. Similarly, visual field changes occur frequently, but shouldn’t be considered progression unless the change is verified in a subsequent (and preferably two) visual fields. Over 80 per cent of abnormal visual fields noted in the Ocular Hypertension Treatment Study were not verified on repeat testing.⁸ Always look for a sustained decrease in visual field results before changing therapy.
Mistake #5: Not getting enough pre-treatment… and post-treatment IOPs
Unless a patient presents with very high IOP (above 45 mmHg) or has advanced disease (with loss of central visual acuity or relative afferent pupil defect in an eye), there is generally no need to rush to treat chronic open angle glaucoma. It is very beneficial to get several IOP readings (at least two and preferably three) before initiating treatment of any kind. At one visit, the patient may be exhibiting a peak IOP or a trough reading. Knowing the range is very important.⁹ Similarly, one should never prematurely judge efficacy of treatment based upon the IOP reading immediately after initiation of therapy.
Even if the first IOP measurement after initiating therapy isn’t impressively lowered, consider leaving therapy unchanged and check at least one more time before deciding if a medication is truly efficacious or not. In the example here, there was an abrupt IOP drop after the initiation of therapy. However, it is notable that there are several pre-treatment IOPs that are nearly identical to the post-treatment IOPs, indicating that the prescribed medication, while overall effective, doesn’t consistently give the robust pressure reduction initially seen (Figure 5).
Figure 5. IOP curve before and after treatment initiation for glaucoma. Several pre-treatment IOPs were nearly identical to post-treatment IOPs, raising questions about the effectiveness of the chosen therapy.
Mistake #6: Not recognising a neurologic visual field in a glaucoma patient
One of the most insidious situations in eye care occurs when a patient with glaucoma manifests a neurologic disease concurrently. While glaucoma causes arcuate visual field defects that respect the horizontal meridian and neurologic conditions cause hemianopic defects that respect the vertical meridian, such patterns can get lost within the same patient. There are two ways to discern these differences. First, a glaucomatous visual field can be predicted by the optic disc and RNFL appearance. When the field loss is greater than expected and, often in an area not anticipated based upon the optic disc appearance, one should look for the neurogenicity by examining carefully both visual fields. Additionally, the greyscale printout is exceptional at identifying visual field defects which respect the vertical meridian while the pattern deviation can be quite poor. Further, while glaucomatous and neurologic damage can occupy the same quadrant, neurological defects may actually manifest a deeper scotoma within a glaucomatous defect.
CASE REPORT
A 74-year-old female previously diagnosed with glaucoma had optic nerve and RNFL damage consistent with glaucoma. However, observation of the grey scale showed bitemporal visual field defects that respected the vertical meridian. The fields were repeated and the pattern persisted. Ultimately, she was diagnosed with a pituitary macroadenoma and scheduled for neurosurgical intervention (Figure 6).
Figure 6. Superior bitemporal visual field defect in a patient with both glaucoma and pituitary macroadenoma. Note that the neurologic field is better appreciated on the grey scale than on the pattern deviation.
A second patient, a 65-year-old female also previously diagnosed with glaucoma exhibited bilateral inferior defects on visual fields. The left visual field matched extreme superior disc damage in that eye. In the right eye, her superior field defect matched optic disc and RNFL damage, but there was no structural abnormality to explain her inferior visual field loss. Most notable was the fact that the right inferior visual field defect stopped at the vertical meridian on the grey scale in the right eye. While the left eye had a significant inferior arcuate scotoma, it was notable that the left inferior nasal defect was absolute and much deeper than the remainder of the field loss. This led to the observation that she had not only glaucomatous arcuate visual field defects, but also a superimposed right inferior quadrantanopia. Subsequent neuroimaging revealed an ischemic cerebral infarct (Figure 7).
Glaucoma diagnosis and management can be quite challenging. It is important to be aware that there are common errors that can make glaucoma management much more challenging.
Figure 7. Right inferior quadrant defect hidden beneath the glaucomatous losses. Note that the neurologic field is better appreciated on the grey scale than on the pattern deviation.
References
1. Ahmad SS. Glaucoma suspects: A practical approach. Taiwan J Ophthalmol 2018; 8: 74-81.
2. Suwan Y, Rettig S, Park SC et al. Effects of Circumpapillary Retinal Nerve Fiber Layer Segmentation Error Correction on Glaucoma Diagnosis in Myopic Eyes. J Glaucoma 2018; 27: 971-975.
3. Giani A, Cigada M, Esmaili DD et al. Artifacts in automatic retinal segmentation using different optical coherence tomography instruments. Retina 2010; 30: 607-616.
4. Miki A, Kumoi M, Usui S et al. Prevalence and Associated Factors of Segmentation Errors in the Peripapillary Retinal Nerve Fiber Layer and Macular Ganglion Cell Complex in Spectral-domain Optical Coherence Tomography Images. J Glaucoma 2017; 26: 995-1000.
5. Chong GT, Lee RK. Glaucoma versus red disease: imaging and glaucoma diagnosis. Curr Opin Ophthalmol 2012; 23: 79-88.
6. Hwang YH, Kim YY, Kim HK et al. Agreement of retinal nerve fiber layer defect location between red-free fundus photography and cirrus HD-OCT maps. Curr Eye Res 2014; 39: 1099-1105.
7. Sayed MS, Margolis M, Lee RK. Green disease in optical coherence tomography diagnosis of glaucoma. Curr Opin Ophthalmol 2017; 28: 139-153.
8. Keltner JL, Johnson CA, Quigg JM et al. Confirmation of visual field abnormalities in the Ocular Hypertension Treatment Study. Ocular Hypertension Treatment Study Group. Arch Ophthalmol 2000; 118: 1187-1194.
9. Durairaj C. Optimal sampling scheme for estimation of intraocular pressure diurnal curves in glaucoma trials. Clin Pharmacokinet 2015; 54: 95-105.
IOP medications available in Australia
A complete list of IOP drops
Download the IOP Medications available in Australia for the management of glaucoma.
The 2024 Student Leadership Program, which ran from 13 March to 10 April, brought together a diverse group of 18 students from across Australia and New Zealand, eager to enhance their leadership skills and make a difference.
A new OV/SA Looking Outward on Optometric Knowledge (LOOK) Local Scholarship has been established to facilitate Australian-based study tours for an OV/SA financial member. The Scholarship is intended to directly improve eye health of local communities throughout Victoria and South Australia.
Optometry Australia is seeking expressions of interest to form an expert Advisory Committee on Digital Health in Optometry (ACDHO). Applications close at 5pm on 19 April 2024.
In the spirit of reconciliation Optometry Australia acknowledges the Traditional Custodians of country throughout Australia and their connections to land, sea and community.
We pay our respects to their Elders past and present and extend that respect to all Aboriginal and Torres Strait Islander peoples today.
Member Login
We use cookies to deliver a better user experience. By selecting 'I accept' you are agreeing to our cookie policy as set out in our Privacy Policy. For more information about the use of cookies and the processing of your personal information, please read our Privacy Policy.I acceptI do not acceptPrivacy policy

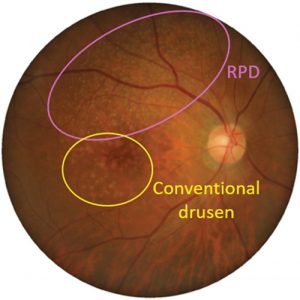
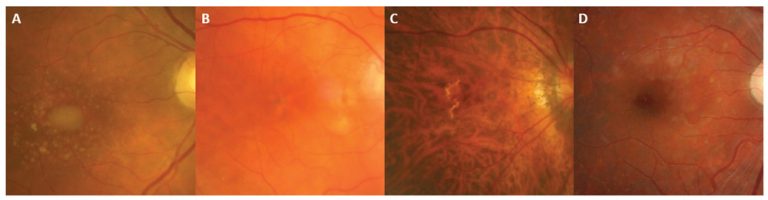
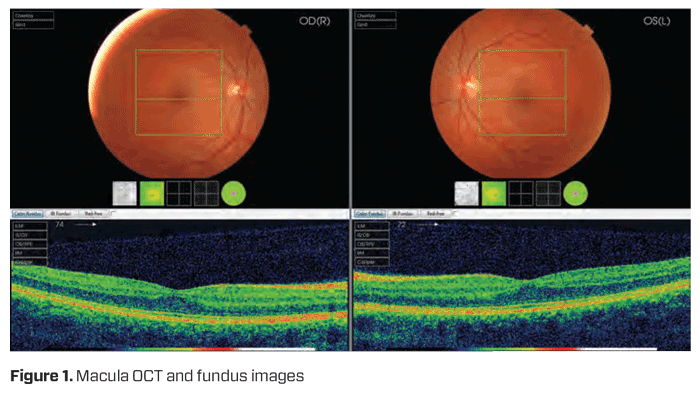
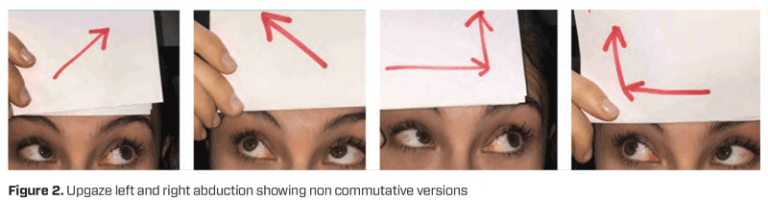
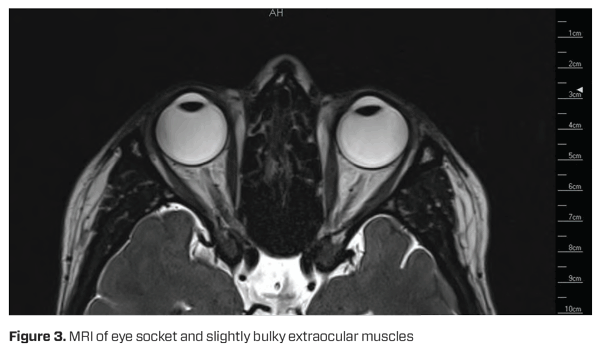
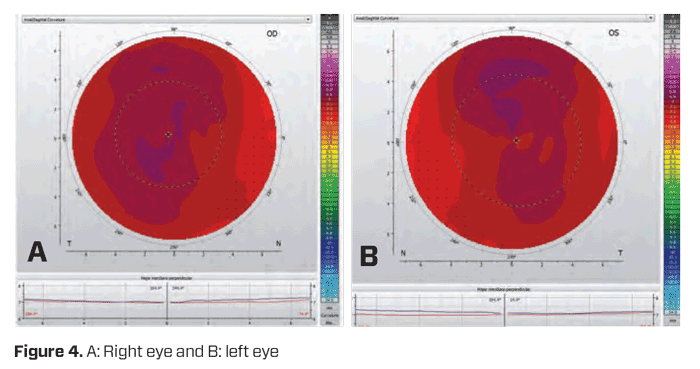

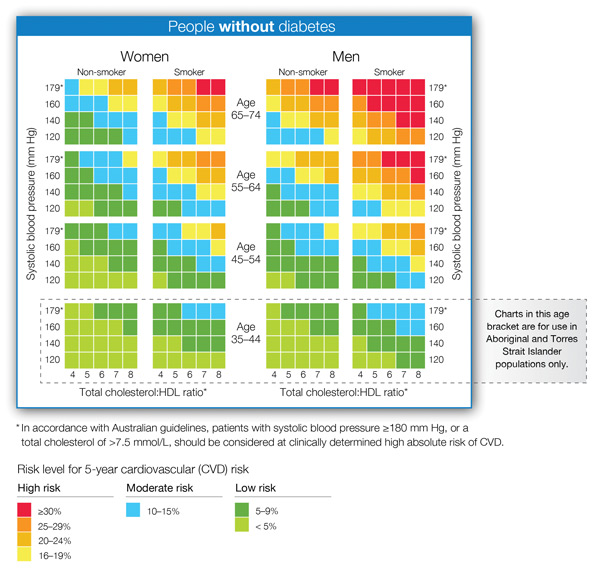
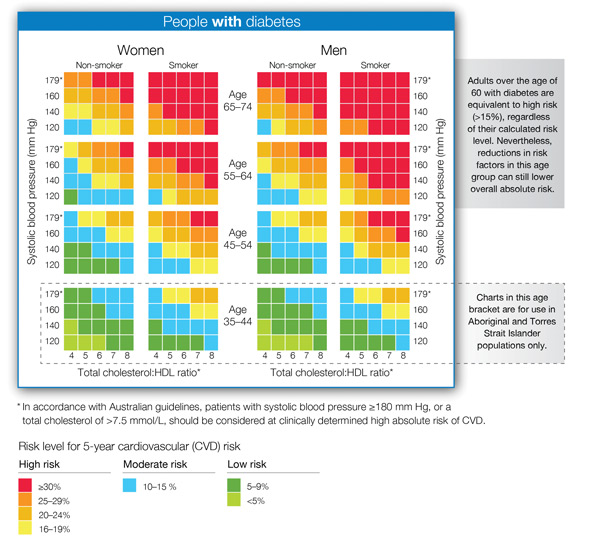
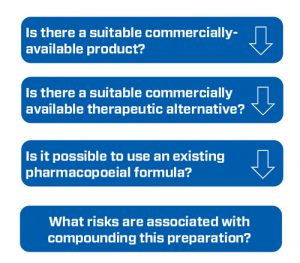
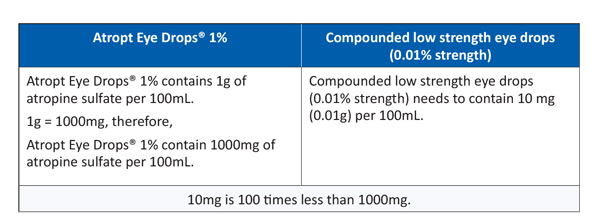
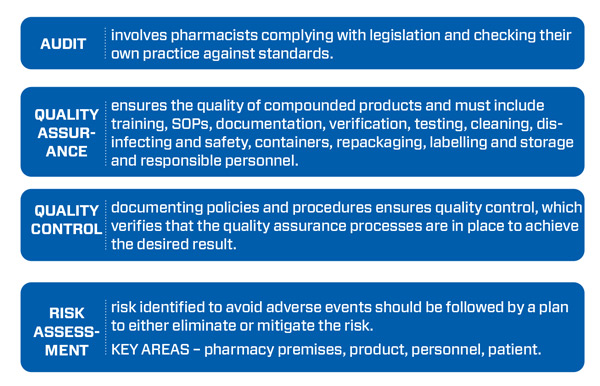
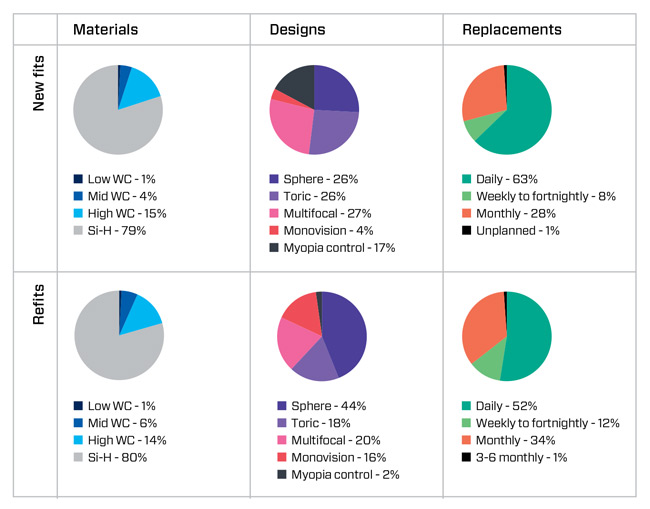
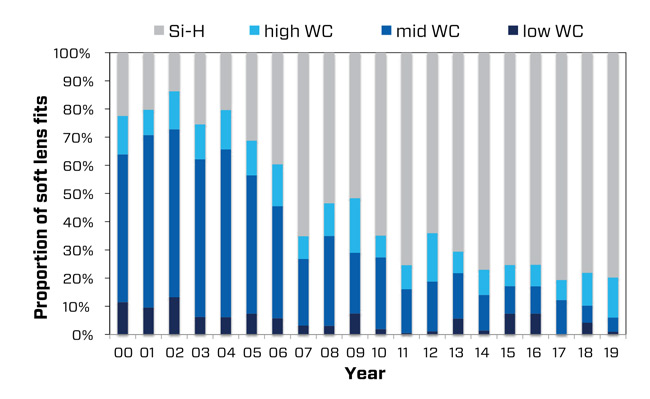
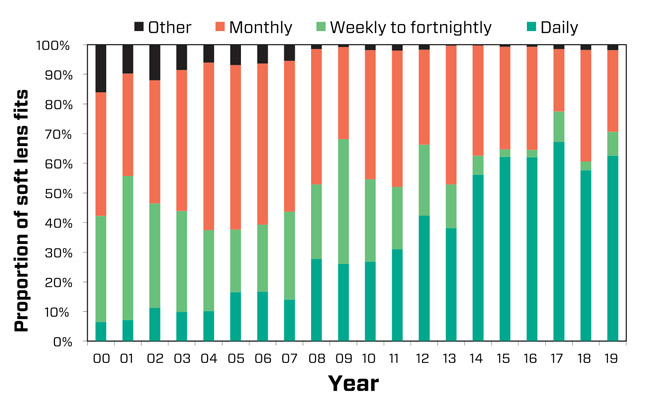
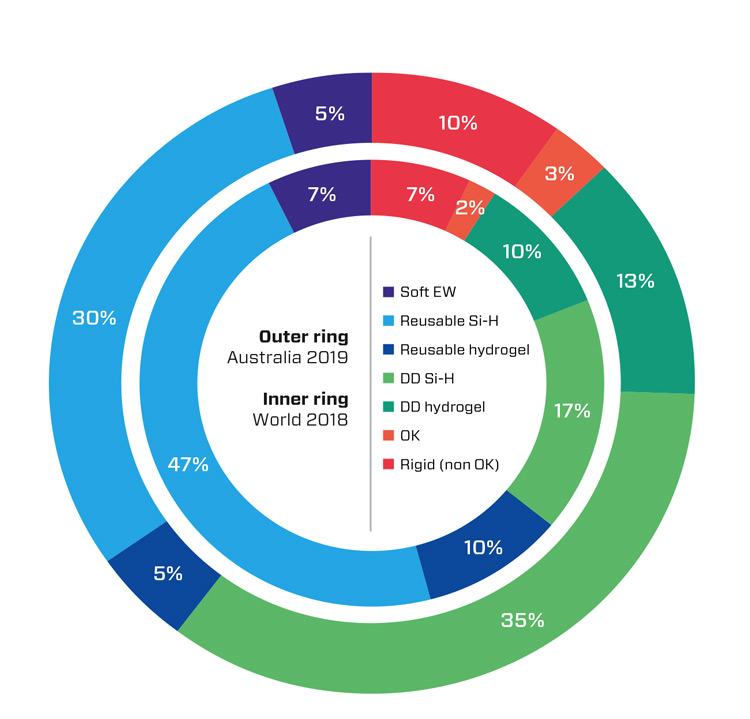
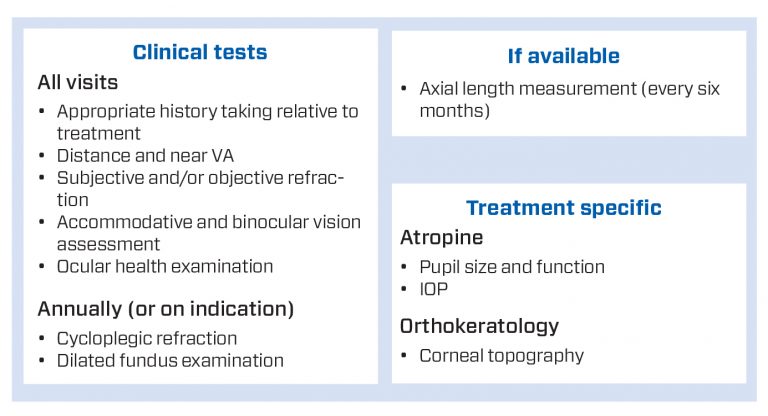
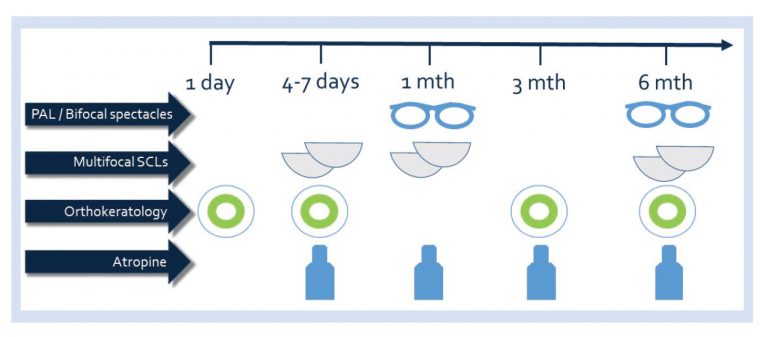
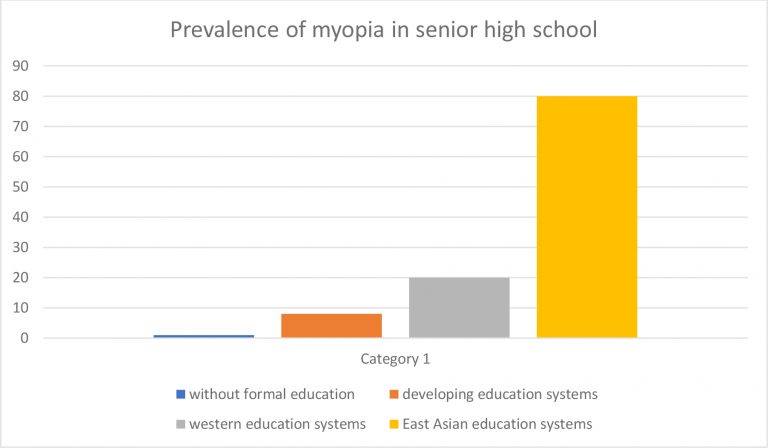
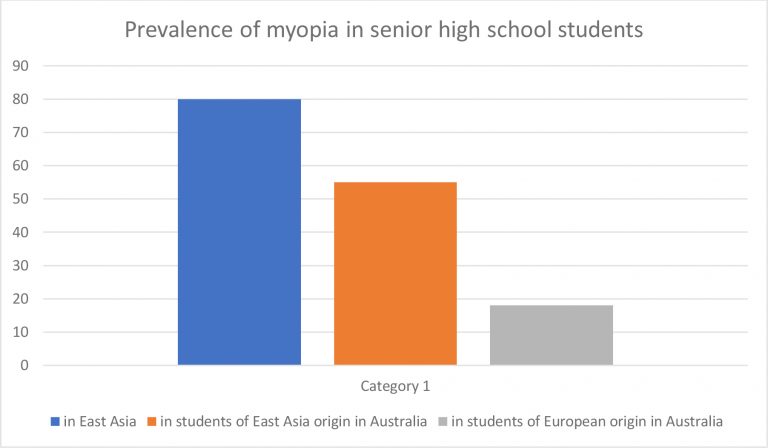
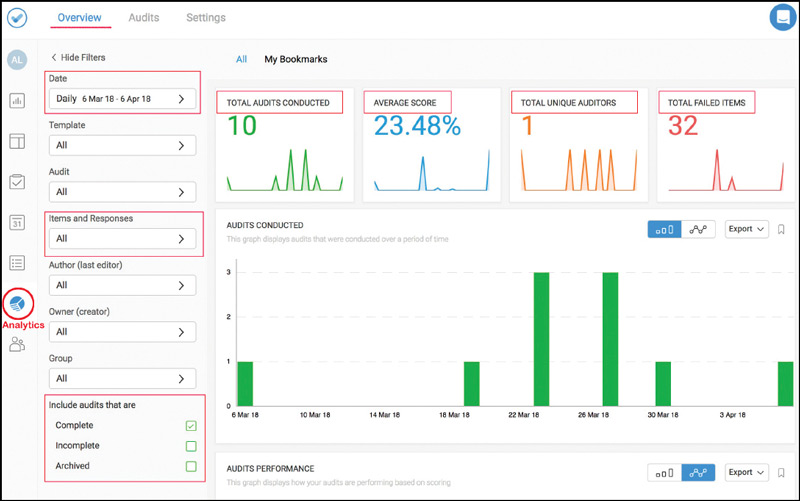
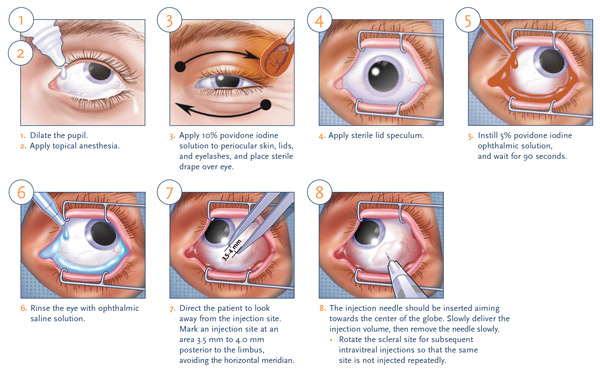
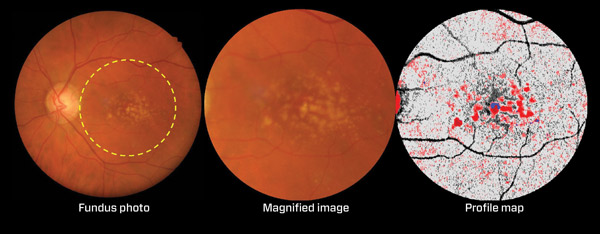

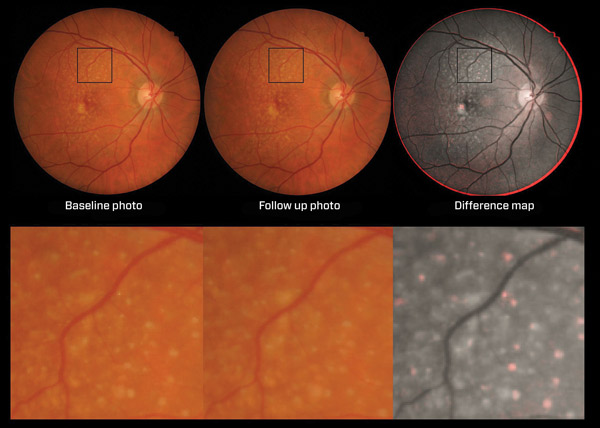
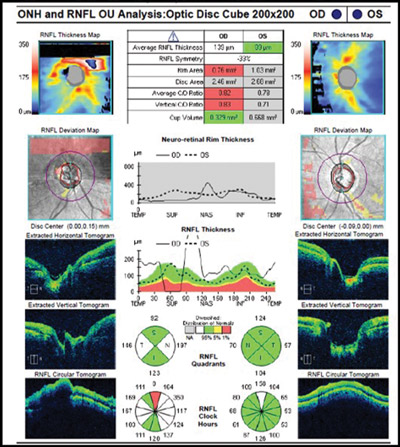
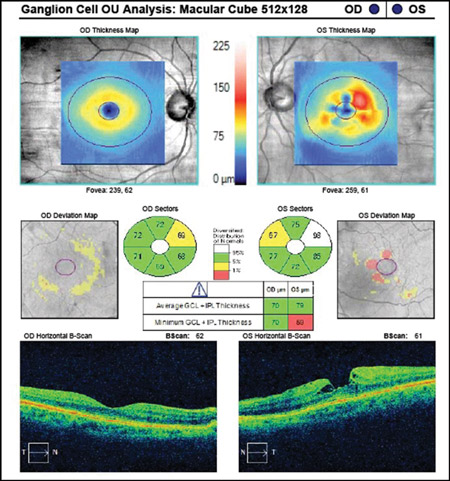
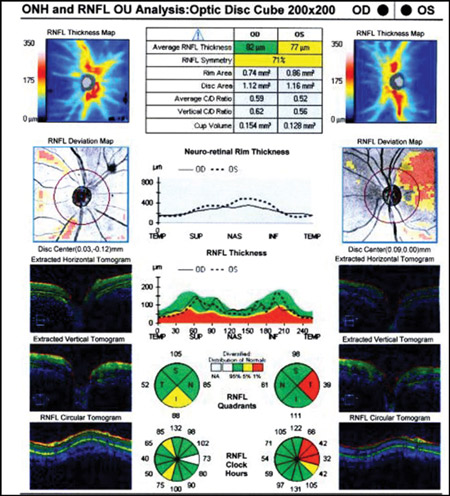
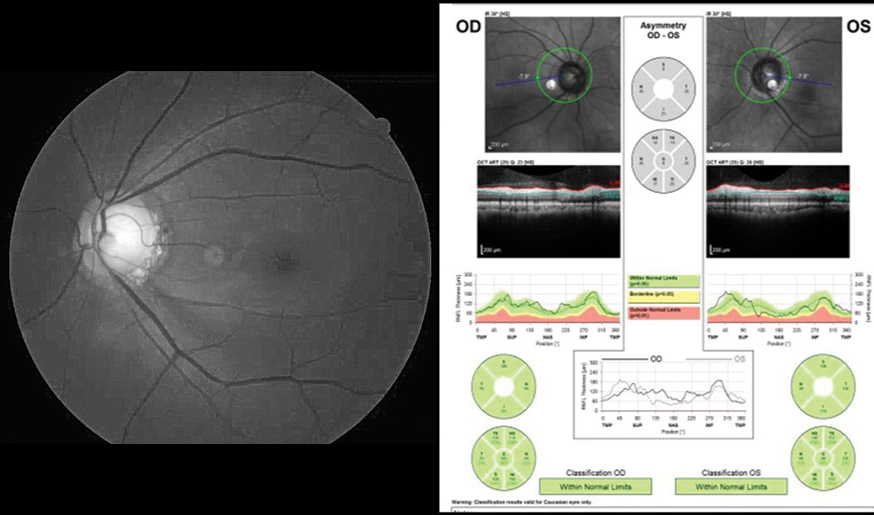
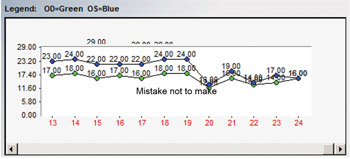
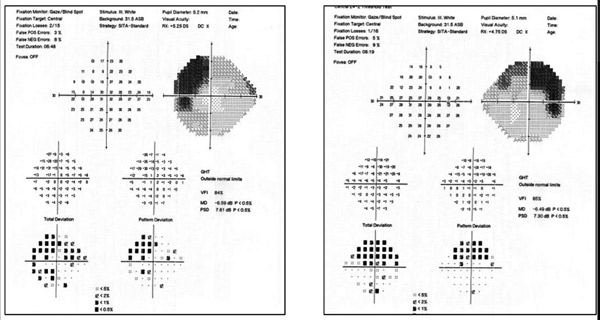
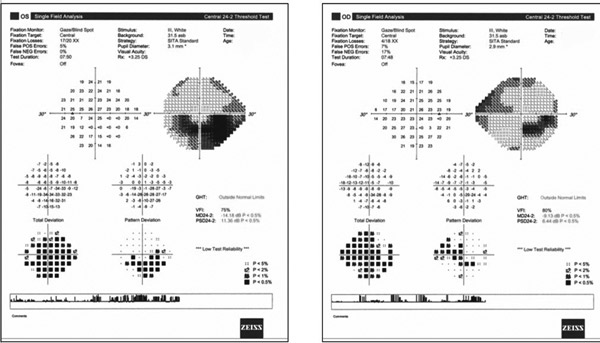

 View
View

